

Malignant tumours of the hand and wrist
- PMID: 22022044
- PMCID: PMC3193646
- DOI: 10.4103/0970-0358.85355
Malignant tumours of the hand and wrist
Abstract
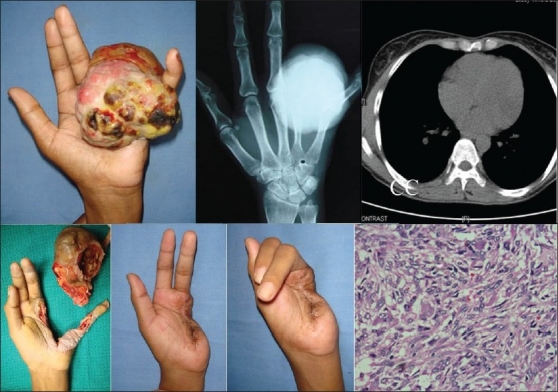
Malignant tumours are rare in the hand and wrist. The clinical presentation may be similar to that of a benign lesion and a high index of suspicion is necessary so that such lesions are not missed by the treating surgeon. Out of a total of 657 tumours/tumour-like lesions of the hand and wrist seen in a tertiary referral centre in a 10-year period, a total of 39 tumours were identified as malignant (5.9%) and of which majority had origin from the skin (53.8%). The management of these tumours is primarily surgical. Limb salvage surgery may be applied when appropriate, though eradication of disease should be the primary goal rather than preservation of function. A multimodal approach is necessary for appropriate management including chemotherapy and radiotherapy.
Keywords: Hand tumours; malignant hand tumours; malignant tumour Rev.
Conflict of interest statement
Figures













References
-
- Mankin HJ, Lange TA, Spanier SS. The hazards of biopsy in patients with malignant primary bone and soft-tissue tumors. J Bone Joint Surg Am. 1982;64:1121–7. - PubMed
-
- Enneking WF, Spanier SS, Goodman MA. A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop Relat Res. 1980;153:106–20. - PubMed
-
- Green FL, Page DL, Fleming ID, Fritz AG, Balch CM, Haller G, et al. 6th edition. New York: Springer-Verlag; 2002. AJCC cancer staging handbook; pp. 213–5.
-
- Wunder J. Musculoskeletal tumors: staging systems., in Orthopaedic knowledge update: musculoskeletal tumors. In: Menendez LR, editor. Rosemont: 2002. pp. 21–7.
-
- Smith RJ. Tumors of the hand: who is best qualified to treat tumors of the hand? J Hand Surg Am. 1977;2:251–2. - PubMed
LinkOut - more resources
Full Text Sources