

Brain morphological signatures for chronic pain
- PMID: 22022493
- PMCID: PMC3192794
- DOI: 10.1371/journal.pone.0026010
Brain morphological signatures for chronic pain
Abstract
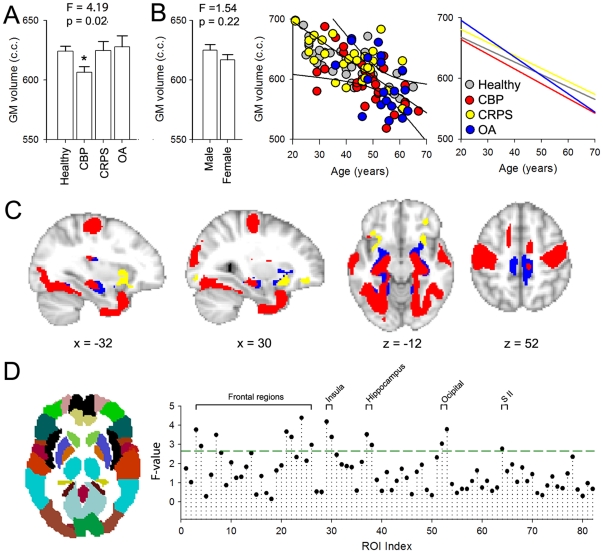
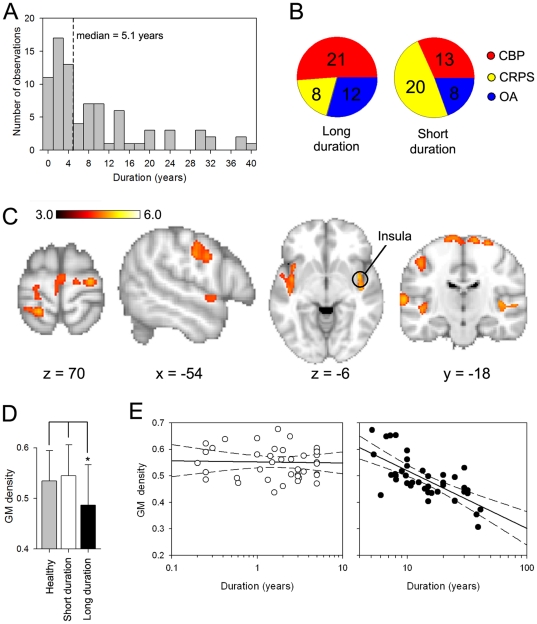
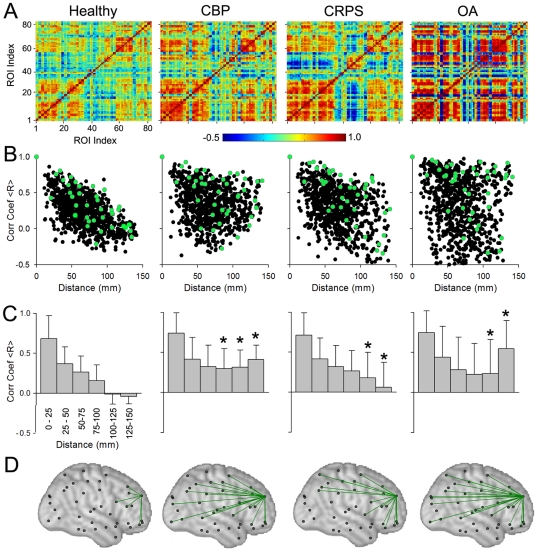
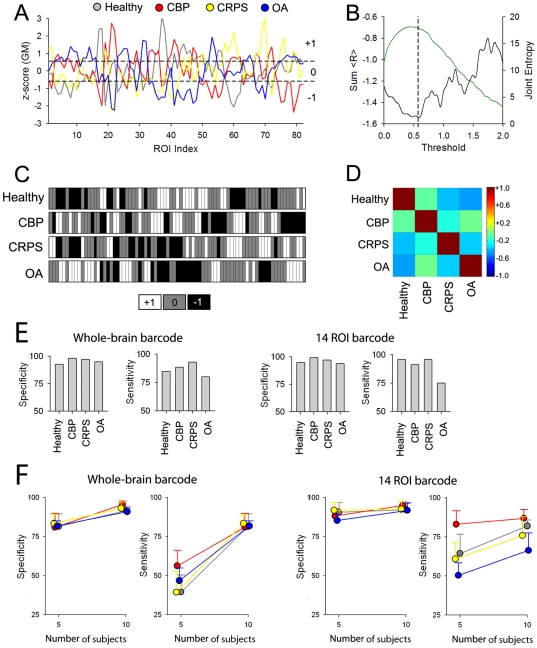
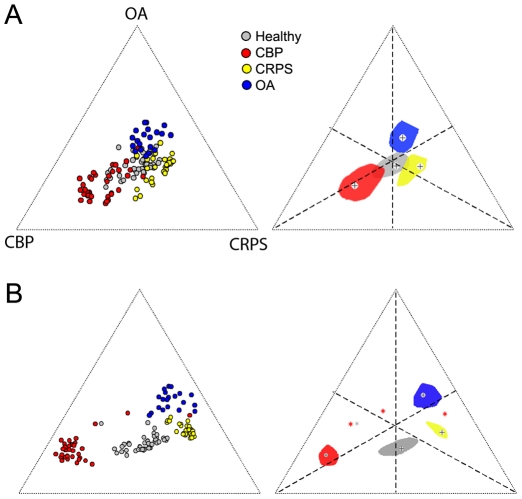
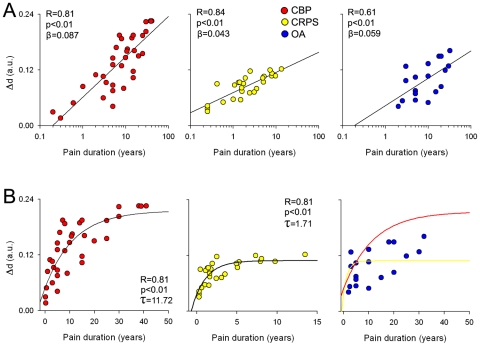
Chronic pain can be understood not only as an altered functional state, but also as a consequence of neuronal plasticity. Here we use in vivo structural MRI to compare global, local, and architectural changes in gray matter properties in patients suffering from chronic back pain (CBP), complex regional pain syndrome (CRPS) and knee osteoarthritis (OA), relative to healthy controls. We find that different chronic pain types exhibit unique anatomical 'brain signatures'. Only the CBP group showed altered whole-brain gray matter volume, while regional gray matter density was distinct for each group. Voxel-wise comparison of gray matter density showed that the impact on the extent of chronicity of pain was localized to a common set of regions across all conditions. When gray matter density was examined for large regions approximating Brodmann areas, it exhibited unique large-scale distributed networks for each group. We derived a barcode, summarized by a single index of within-subject co-variation of gray matter density, which enabled classification of individual brains to their conditions with high accuracy. This index also enabled calculating time constants and asymptotic amplitudes for an exponential increase in brain re-organization with pain chronicity, and showed that brain reorganization with pain chronicity was 6 times slower and twice as large in CBP in comparison to CRPS. The results show an exuberance of brain anatomical reorganization peculiar to each condition and as such reflecting the unique maladaptive physiology of different types of chronic pain.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
