

Interfacility helicopter ambulance transport of neurosurgical patients: observations, utilization, and outcomes from a quaternary level care hospital
- PMID: 22022572
- PMCID: PMC3192167
- DOI: 10.1371/journal.pone.0026216
Interfacility helicopter ambulance transport of neurosurgical patients: observations, utilization, and outcomes from a quaternary level care hospital
Abstract
Background: The clinical benefit of helicopter transport over ground transportation for interfacility transport is unproven. We sought to determine actual practice patterns, utilization, and outcomes of patients undergoing interfacility transport for neurosurgical conditions.
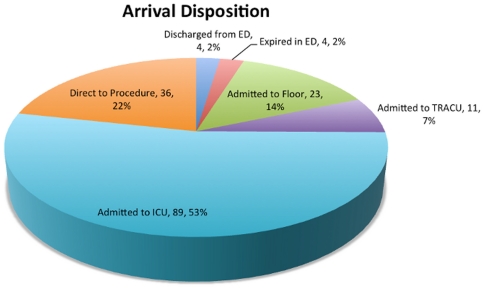
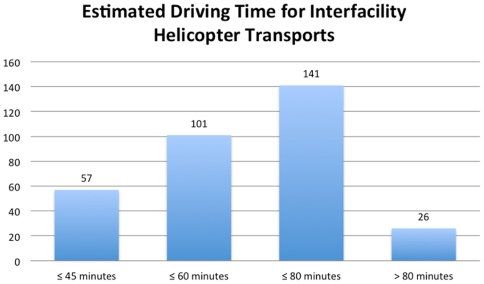
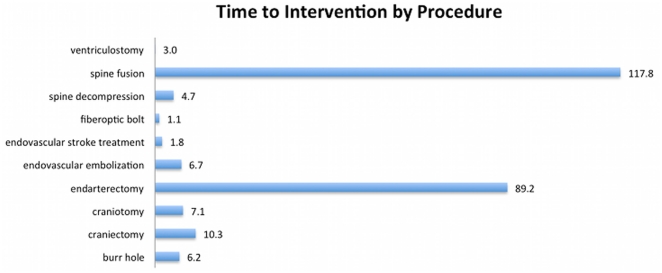
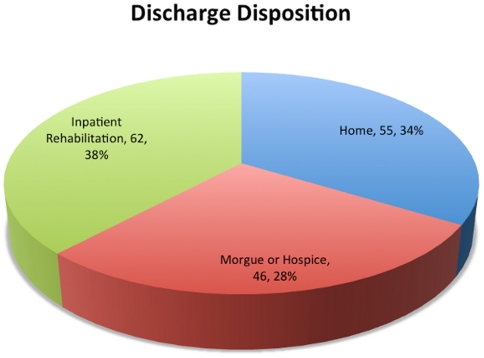
Methodology/principal findings: We retrospectively examined all interfacility helicopter transfers to a single trauma center during 2008. We restricted our analysis to those transfers leading either to admission to the neurosurgical service or to formal consultation upon arrival. Major exclusion criteria included transport from the scene, death during transport, and transport to any area of the hospital other than the emergency department. The primary outcome was time interval to invasive intervention. Secondary outcomes were estimated ground transportation times from the referring hospital, admitting disposition, and discharge disposition. Of 526 candidate interfacility helicopter transfers to our emergency department in 2008, we identified 167 meeting study criteria. Seventy-five (45%) of these patients underwent neurosurgical intervention. The median time to neurosurgical intervention ranged from 1.0 to 117.8 hours, varying depending on the diagnosis. For 101 (60%) of the patients, estimated driving time from the referring institution was less than one hour. Four patients (2%) expired in the emergency department, and 34 patients (20%) were admitted to a non-ICU setting. Six patients were discharged home within 24 hours. For those admitted, in-hospital mortality was 28%.
Conclusions/significance: Many patients undergoing interfacility transfer for neurosurgical evaluation are inappropriately triaged to helicopter transport, as evidenced by actual times to intervention at the accepting institution and estimated ground transportation times from the referring institution. In a time when there is growing interest in health care cost containment, practitioners must exercise discretion in the selection of patients for air ambulance transport--particularly when it may not bear influence on clinical outcome. Neurosurgical evaluation via telemedicine may be one strategy for improving air transport triage.
Conflict of interest statement
Figures
References
-
- Southard PA, Hedges JR, Hunter JG, Ungerleider RM. Impact of a Transfer Center on Interhospital Referrals and Transfers to a Tertiary Care Center. Academic Emergency Medicine. 2005;12:653–657. - PubMed
-
- Spain DA, Bellino M, Kopelman A, Chang J, Park J, et al. Requests for 692 transfers to an academic level I trauma center: implications of the emergency medical treatment and active labor act. J Trauma. 2007;62:63–67. discussion 67–68. - PubMed
-
- Babu MA, Nahed BV, Demoya MM, Curry WT. Is Trauma Transfer Influenced by Factors Other than Medical Need? An Examination of Insurance Status and Transfer in Patients with Mild Head Injury. Neurosurgery. 2011. Available: http://www.ncbi.nlm.nih.gov/pubmed/21499151. - PubMed
-
- Sasser SM, Hunt RC, Sullivent EE, Wald MM, Mitchko J, et al. Guidelines for field triage of injured patients. Recommendations of the National Expert Panel on Field Triage. MMWR Recomm Rep. 2009;58:1–35. - PubMed
-
- Arfken CL, Shapiro MJ, Bessey PQ, Littenberg B. Effectiveness of helicopter versus ground ambulance services for interfacility transport. J Trauma. 1998;45:785–790. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
