

Schistosomiasis and soil-transmitted helminth control in Niger: cost effectiveness of school based and community distributed mass drug administration [corrected]
- PMID: 22022622
- PMCID: PMC3191121
- DOI: 10.1371/journal.pntd.0001326
Schistosomiasis and soil-transmitted helminth control in Niger: cost effectiveness of school based and community distributed mass drug administration [corrected]
Erratum in
- PLoS Negl Trop Dis. 2012 Apr;6(4): doi/10.1371/annotation/30823662-77ac-4ac3-bd32-6f300121ac3f
- PLoS Negl Trop Dis. 2012 Apr;6(4): doi/10.1371/annotation/d9dce505-07d7-4d19-8c2f-9f707bddc287
Abstract
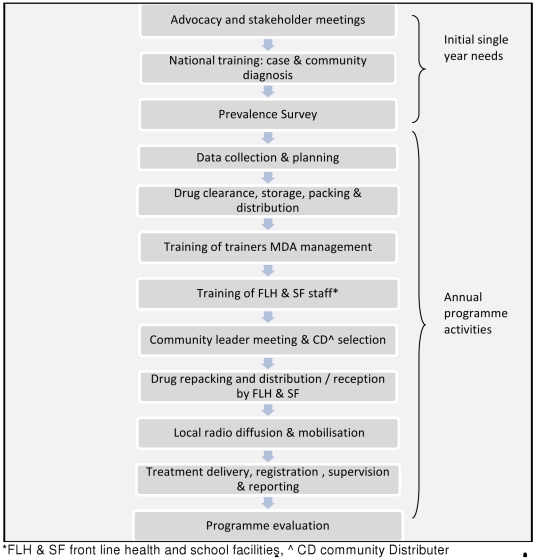
Background: In 2004 Niger established a large scale schistosomiasis and soil-transmitted helminths control programme targeting children aged 5-14 years and adults. In two years 4.3 million treatments were delivered in 40 districts using school based and community distribution.
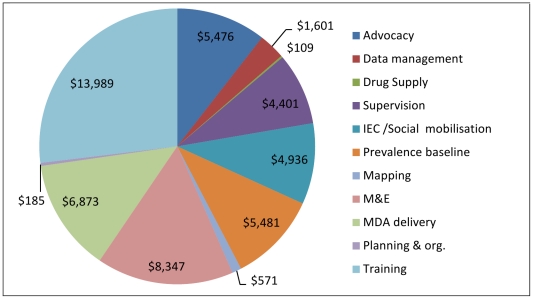
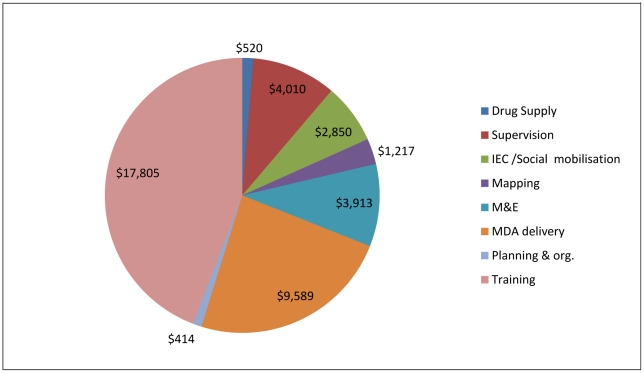
Method and findings: Four districts were surveyed in 2006 to estimate the economic cost per district, per treatment and per schistosomiasis infection averted. The study compares the costs of treatment at start up and in a subsequent year, identifies the allocation of costs by activity, input and organisation, and assesses the cost of treatment. The cost of delivery provided by teachers is compared to cost of delivery by community distributers (CDD). The total economic cost of the programme including programmatic, national and local government costs and international support in four study districts, over two years, was US$ 456,718; an economic cost/treatment of $0.58. The full economic delivery cost of school based treatment in 2005/06 was $0.76, and for community distribution was $0.46. Including only the programme costs the figures are $0.47 and $0.41 respectively. Differences at sub-district are more marked. This is partly explained by the fact that a CDD treats 5.8 people for every one treated in school. The range in cost effectiveness for both direct and direct and indirect treatments is quantified and the need to develop and refine such estimates is emphasised.
Conclusions: The relative cost effectiveness of school and community delivery differs by country according to the composition of the population treated, the numbers targeted and treated at school and in the community, the cost and frequency of training teachers and CDDs. Options analysis of technical and implementation alternatives including a financial analysis should form part of the programme design process.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Canning D. Priority setting and the ‘neglected’ tropical diseases. Transactions of the Royal Society of Tropical Medicine and Hygiene. 2006;100:499–504. - PubMed
-
- Walker D, Fox-Rushby J. Economic evaluation of parasitic diseases: A critique of the internal and external validity of published studies. Tropical Medicine and International Health. 2000;5/4:237–249. - PubMed
-
- Gabrielli AF, Touré S, Sellin B, Sellin E, Ky C, et al. A combined school- and community-based campaign targeting all school-age children of Burkina Faso against schistosomiasis and soil-transmitted helminthiasis: Performance, financial costs and implications for sustainability. Acta Tropica. 2006;99:234–242. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
