

Emerging trends in Lassa fever: redefining the role of immunoglobulin M and inflammation in diagnosing acute infection
- PMID: 22023795
- PMCID: PMC3223505
- DOI: 10.1186/1743-422X-8-478
Emerging trends in Lassa fever: redefining the role of immunoglobulin M and inflammation in diagnosing acute infection
Abstract
Background: Lassa fever (LF) is a devastating hemorrhagic viral disease that is endemic to West Africa and responsible for thousands of human deaths each year. Analysis of humoral immune responses (IgM and IgG) by antibody-capture ELISA (Ab-capture ELISA) and Lassa virus (LASV) viremia by antigen-capture ELISA (Ag-capture ELISA) in suspected patients admitted to the Kenema Government Hospital (KGH) Lassa Fever Ward (LFW) in Sierra Leone over the past five years is reshaping our understanding of acute LF.
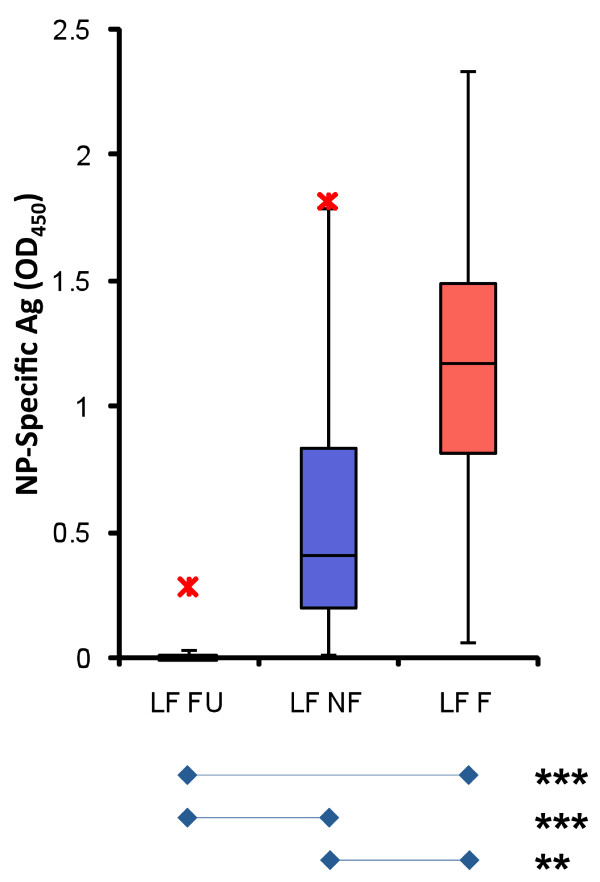
Results: Analyses in LF survivors indicated that LASV-specific IgM persists for months to years after initial infection. Furthermore, exposure to LASV appeared to be more prevalent in historically non-endemic areas of West Africa with significant percentages of reportedly healthy donors IgM and IgG positive in LASV-specific Ab-capture ELISA. We found that LF patients who were Ag positive were more likely to die than suspected cases who were only IgM positive. Analysis of metabolic and immunological parameters in Ag positive LF patients revealed a strong correlation between survival and low levels of IL-6, -8, -10, CD40L, BUN, ALP, ALT, and AST. Despite presenting to the hospital with fever and in some instances other symptoms consistent with LF, the profiles of Ag negative IgM positive individuals were similar to those of normal donors and nonfatal (NF) LF cases, suggesting that IgM status cannot necessarily be considered a diagnostic marker of acute LF in suspected cases living in endemic areas of West Africa.
Conclusion: Only LASV viremia assessed by Ag-capture immunoassay, nucleic acid detection or virus isolation should be used to diagnose acute LASV infection in West Africans. LASV-specific IgM serostatus cannot be considered a diagnostic marker of acute LF in suspected cases living in endemic areas of West Africa. By applying these criteria, we identified a dysregulated metabolic and pro-inflammatory response profile conferring a poor prognosis in acute LF. In addition to suggesting that the current diagnostic paradigm for acute LF should be reconsidered, these studies present new opportunities for therapeutic interventions based on potential prognostic markers in LF.
Figures




References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
