

Controlled comparison of family cognitive behavioral therapy and psychoeducation/relaxation training for child obsessive-compulsive disorder
- PMID: 22024003
- PMCID: PMC3205429
- DOI: 10.1016/j.jaac.2011.08.003
Controlled comparison of family cognitive behavioral therapy and psychoeducation/relaxation training for child obsessive-compulsive disorder
Abstract
Objective: To examine the efficacy of exposure-based cognitive-behavioral therapy (CBT) plus a structured family intervention (FCBT) versus psychoeducation plus relaxation training (PRT) for reducing symptom severity, functional impairment, and family accommodation in youths with obsessive-compulsive disorder (OCD).
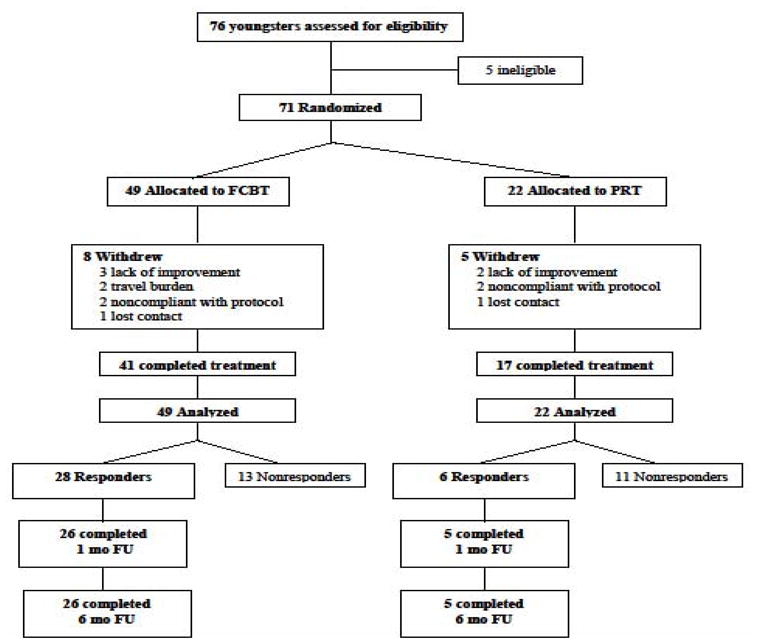
Method: A total of 71 youngsters 8 to 17 years of age (mean 12.2 years; range, 8-17 years, 37% male, 78% Caucasian) with primary OCD were randomized (70:30) to 12 sessions over 14 weeks of FCBT or PRT. Blind raters assessed outcomes with responders followed for 6 months to assess treatment durability.
Results: FCBT led to significantly higher response rates than PRT in ITT (57.1% vs 27.3%) and completer analyses (68.3% vs. 35.3%). Using HLM, FCBT was associated with significantly greater change in OCD severity and child-reported functional impairment than PRT and marginally greater change in parent-reported accommodation of symptoms. These findings were confirmed in some, but not all, secondary analyses. Clinical remission rates were 42.5% for FCBT versus 17.6% for PRT. Reduction in family accommodation temporally preceded improvement in OCD for both groups and child functional status for FCBT only. Treatment gains were maintained at 6 months.
Conclusions: FCBT is effective for reducing OCD severity and impairment. Importantly, treatment also reduced parent-reported involvement in symptoms with reduced accommodation preceding reduced symptom severity and functional impairment. CLINICAL TRIALS REGISTRY INFORMATION: Behavior Therapy for Children and Adolescents with Obsessive-Compulsive Disorder (OCD); http://www.clinicaltrials.gov; NCT00000386.
Copyright © 2011 American Academy of Child and Adolescent Psychiatry. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Piacentini J, Bergman RL, Keller M, McCracken J. Functional impairment in children and adolescents with Obsessive Compulsive Disorder. J Child Adol Psychopharmacology. 2003;13:61–70. - PubMed
-
- Storch EA, Larson MJ, Muroff J, et al. Predictors of functional impairment in pediatric obsessive-compulsive disorder. J Anxiety Disord. 2010;24:275–283. - PubMed
-
- Moore PS, Mariaski A, March J, et al. Obsessive-compulsive disorder in children and adolescents: Diagnosis, comorbidity, and developmental factors. Handbook of child and adolescent obsessive-compulsive disorder. 2007:17–45.
-
- Barrett P, Farrell L, Pina A, Peris TS, Piacentini J. Evidence-based treatments for child and adolescent OCD. J Clin Child Adolesc Psychol. 2008;37:131–155. - PubMed
-
- Geller D, Biederman J, Stewart S, et al. Which SSRI? A meta-analysis of pharmacotherapy trials for pediatric obsessive compulsive disorder. Am J Psychiatry. 2003;160:1919–1928. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
