

Neural correlates of reversal learning in severe mood dysregulation and pediatric bipolar disorder
- PMID: 22024005
- PMCID: PMC3206630
- DOI: 10.1016/j.jaac.2011.07.011
Neural correlates of reversal learning in severe mood dysregulation and pediatric bipolar disorder
Abstract
Objective: Outcome and family history data differentiate children with severe mood dysregulation (SMD), a syndrome characterized by chronic irritability, from children with "classic" episodic bipolar disorder (BD). Nevertheless, the presence of cognitive inflexibility in SMD and BD highlights the need to delineate neurophysiologic similarities and differences between the two patient groups. Functional magnetic resonance imaging was used to examine neural correlates of cognitive flexibility deficits in patients with SMD and BD versus healthy volunteers (HV).
Method: During functional magnetic resonance imaging, subjects completed a response reversal task that assessed cognitive flexibility (n = 22 with SMD, 26 with BD, 34 HV). Task effects were examined in four regions of interest: caudate, cingulate gyrus, inferior frontal gyrus (IFG), and ventromedial prefrontal cortex.
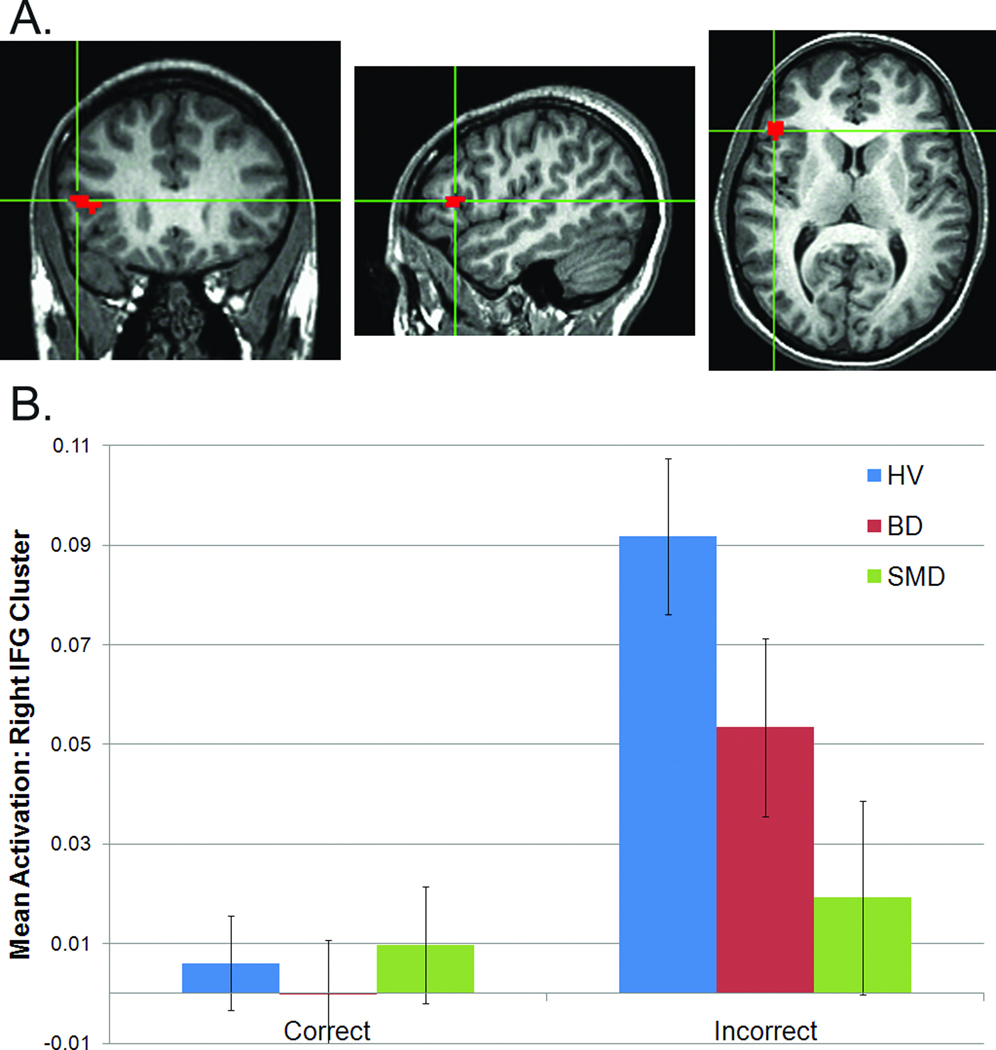
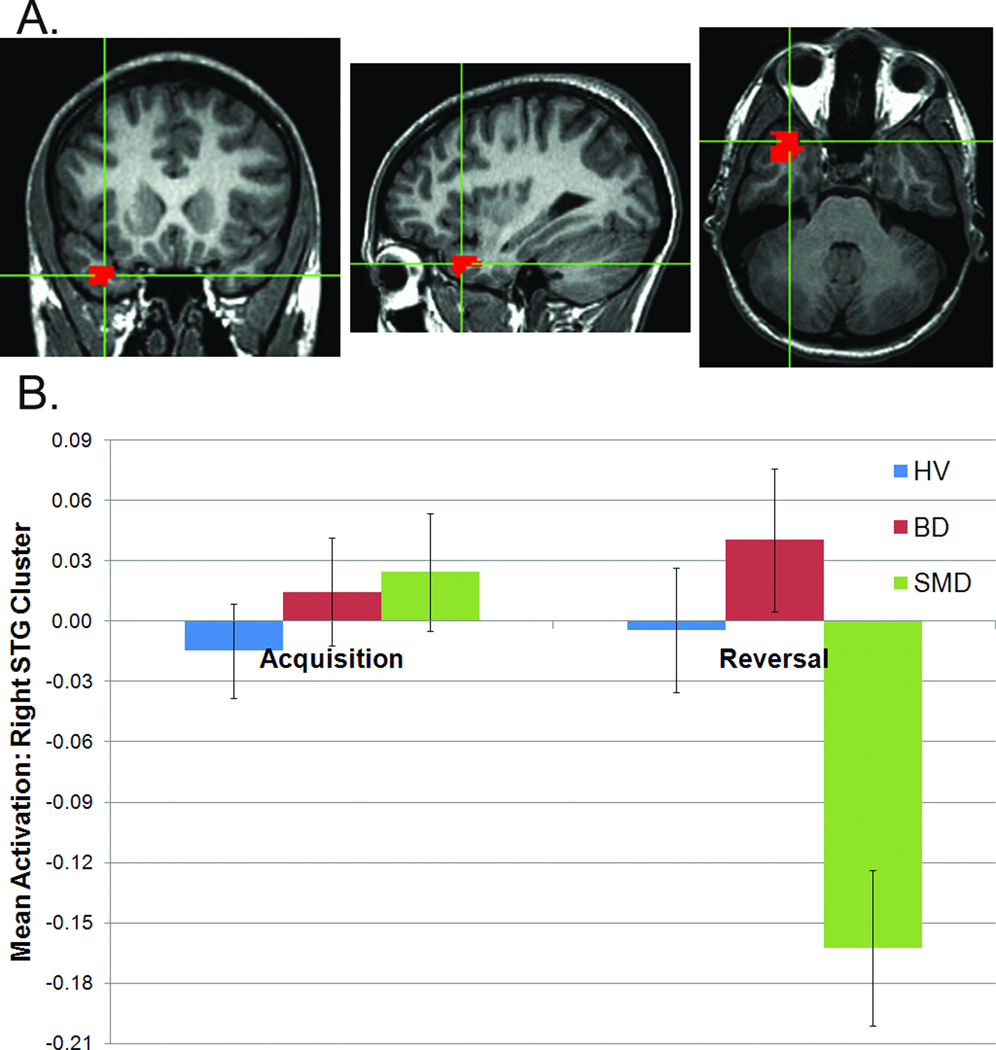
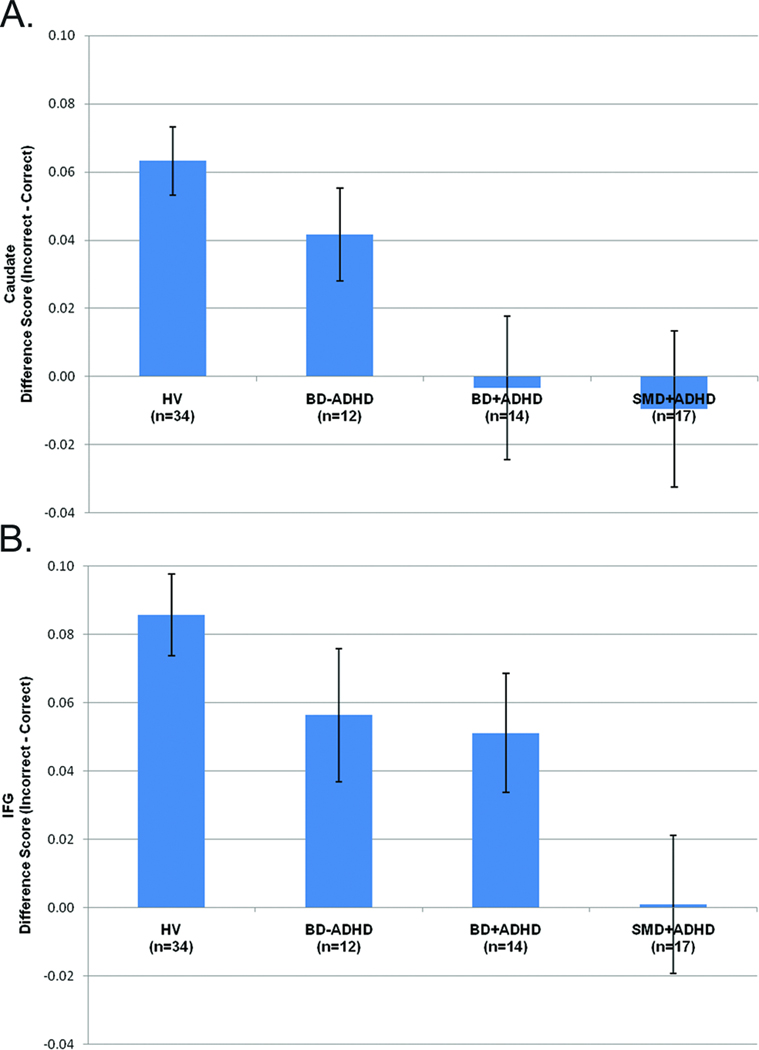
Results: Diagnosis-by-accuracy interactions emerged in the caudate and IFG. In these regions, the difference in activation was calculated between incorrect and correct trials. In the caudate, this value was smaller in subjects with SMD and with BD than in HV. In the IFG, however, this value was smaller in subjects with SMD than in those with BD and in HV. Post hoc analyses indicated that comorbid attention-deficit/hyperactivity disorder in patients may influence the caudate findings. Exploratory whole-brain analysis confirmed the caudate and IFG findings. In addition, other regions differentiating SMD from BD were identified (e.g., superior parietal lobule/precuneus and inferior temporal gyrus).
Conclusions: In response to errors, similar perturbations occur in the caudate for youth with SMD and BD compared with HV youth. IFG deficits, in contrast, manifest in youth with SMD, but not with BD.
Copyright © 2011 American Academy of Child and Adolescent Psychiatry. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures

References
-
- Leibenluft E, Charney DS, Towbin KE, Bhangoo RK, Pine DS. Defining clinical phenotypes of juvenile mania. Am J Psychiatry. 2003;160(3):430–437. - PubMed
-
- Brotman MA, Kassem L, Reising MM, et al. Parental diagnoses in youth with narrow phenotype bipolar disorder or severe mood dysregulation. Am J Psychiatry. 2007;164(8):1238–1241. - PubMed
-
- Brotman MA, Schmajuk M, Rich BA, et al. Prevalence, clinical correlates, and longitudinal course of severe mood dysregulation in children. Biol Psychiatry. 2006;60(9):991–997. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
