

Use of diffusion tensor MRI to identify early changes in diabetic nephropathy
- PMID: 22024476
- PMCID: PMC3214881
- DOI: 10.1159/000333044
Use of diffusion tensor MRI to identify early changes in diabetic nephropathy
Abstract
Background/aims: Currently available clinical indicators of kidney disease lack the sensitivity and/or specificity to identify early-stage diabetic nephropathy (DN). Quantitative diffusion magnetic resonance imaging (MRI), specifically diffusion tensor imaging (DTI), has been used to quantify pathophysiologic changes in other organs but has not been well studied in kidney diseases, including DN. The goal of this pilot study was to examine differences in kidney DTI parameters in diabetic subjects versus healthy controls.
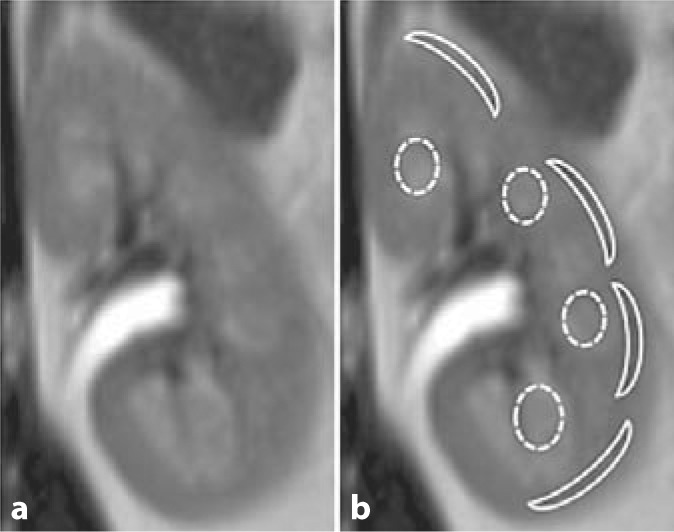
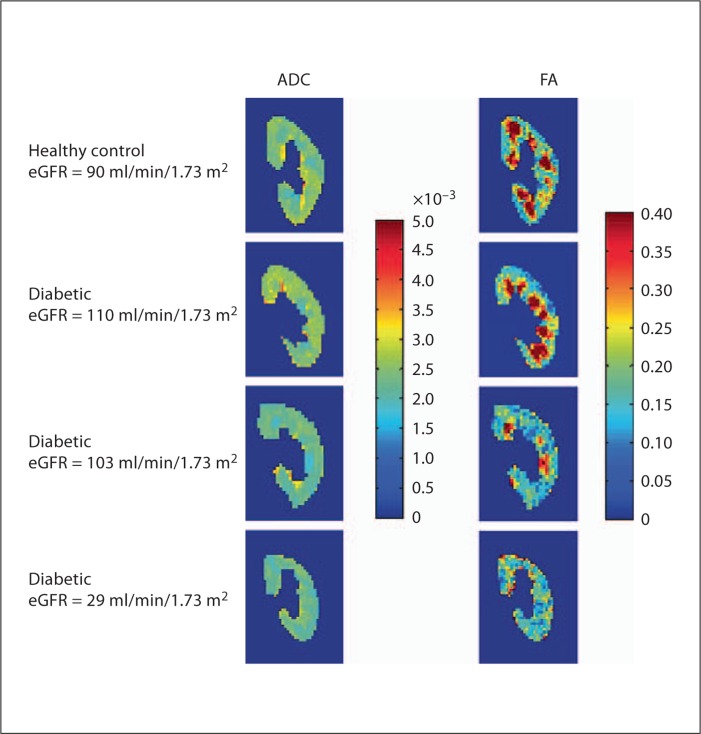
Methods: 16 diabetic and 5 healthy control subjects were recruited for this institutional review board-approved/Health Insurance Portability and Accountability Act-compliant study. Kidneys were scanned using DTI to generate apparent diffusion coefficient (ADC) and fractional anisotropy (FA) data. Mean cortical and medullary ADC and FA values were calculated by selecting multiple regions of interest. Diabetics were stratified by estimated glomerular filtration rate (eGFR) into 2 groups: eGFR ≥60 (n = 10) and eGFR <60 (n = 6) ml/min/1.73 m(2). Mean diffusion parameters and eGFRs were compared between these groups of diabetic subjects and healthy controls.
Results: Medullary FA, ADC and cortical ADC values were significantly lower in diabetics with eGFR <60 compared to controls. Notably, both mean medullary FA and ADC were significantly lower in diabetics with eGFR ≥60 compared to controls (p = 0.001 and p = 0.042, respectively). For the study subjects in aggregate, medullary FA correlated significantly with eGFR (R = 0.69, p < 0.01); the other diffusion parameters showed no significant correlations.
Conclusions: This pilot study suggests that changes in medullary DTI assessments may serve as indicators of early DN. Further studies are needed to determine if these findings could serve as biomarkers to identify diabetics at risk of DN progression.
Copyright © 2011 S. Karger AG, Basel.
Figures

References
-
- Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27:1047–1053. - PubMed
-
- Retnakaran R, Cull CA, Thorne KI, Adler AI, Holman RR. Risk factors for renal dysfunction in type 2 diabetes: UK Prospective diabetes study 74. Diabetes. 2006;55:1832–1839. - PubMed
-
- Basser PJ, Mattiello J, LeBihan D. Estimation of the effective self-diffusion tensor from the NMR spin-echo. J Magn Reson B. 1994;103:247–254. - PubMed
-
- Chandarana H, Lee VS. Renal functional MRI: are we ready for clinical application? AJR Am J Roentgenol. 2009;192:1550–1557. - PubMed
-
- Huang AJ, Lee VS, Rusinek H. MR imaging of renal function. Radiol Clin North Am. 2003;41:1001–1017. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
