

Performance of the traditional age, sex, and angina typicality-based approach for estimating pretest probability of angiographically significant coronary artery disease in patients undergoing coronary computed tomographic angiography: results from the multinational coronary CT angiography evaluation for clinical outcomes: an international multicenter registry (CONFIRM)
- PMID: 22025600
- PMCID: PMC3240578
- DOI: 10.1161/CIRCULATIONAHA.111.039255
Performance of the traditional age, sex, and angina typicality-based approach for estimating pretest probability of angiographically significant coronary artery disease in patients undergoing coronary computed tomographic angiography: results from the multinational coronary CT angiography evaluation for clinical outcomes: an international multicenter registry (CONFIRM)
Abstract
Background: Guidelines for the management of patients with suspected coronary artery disease (CAD) rely on the age, sex, and angina typicality-based pretest probabilities of angiographically significant CAD derived from invasive coronary angiography (guideline probabilities). Reliability of guideline probabilities has not been investigated in patients referred to noninvasive CAD testing.
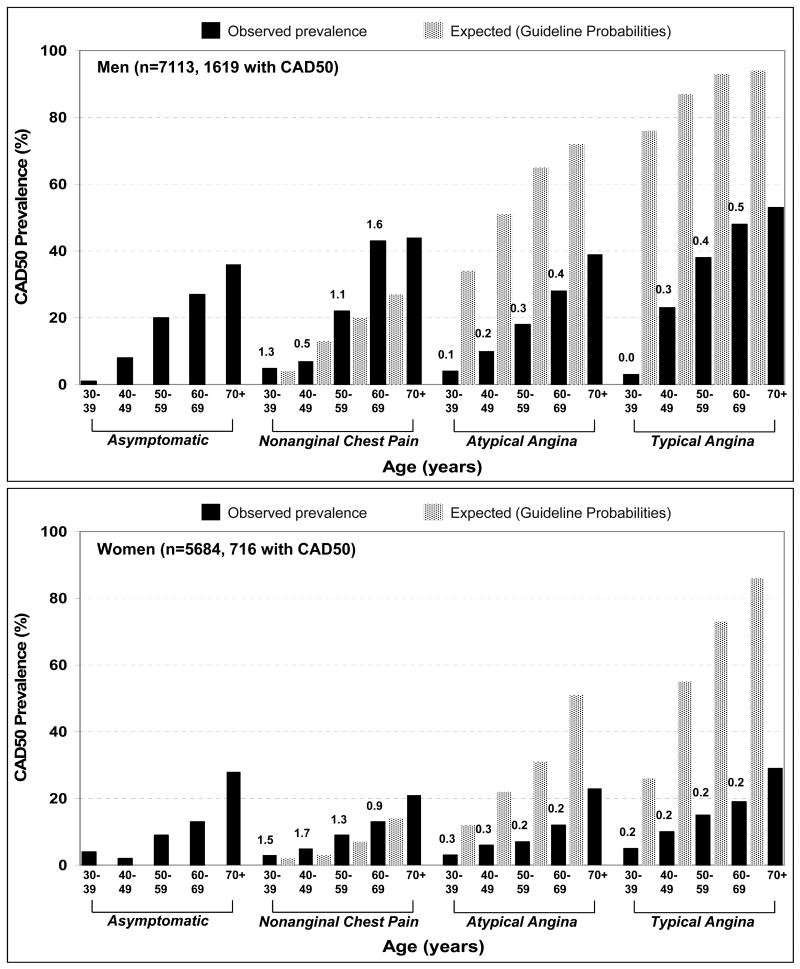
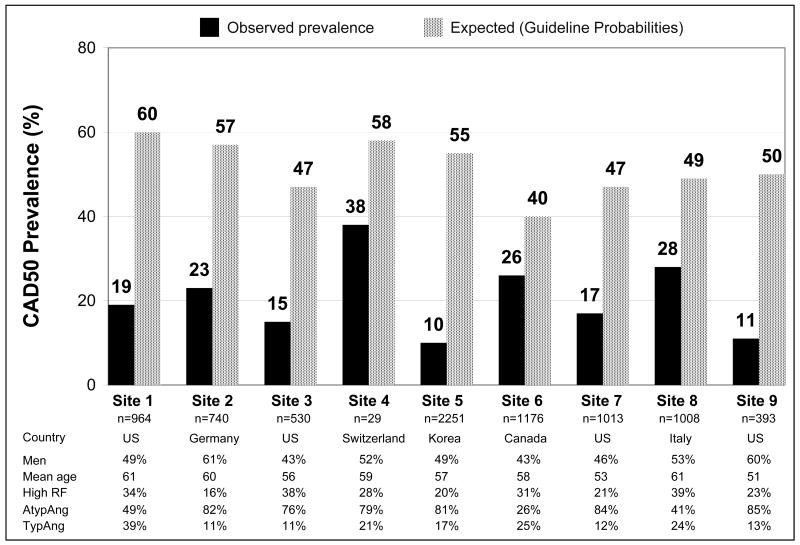
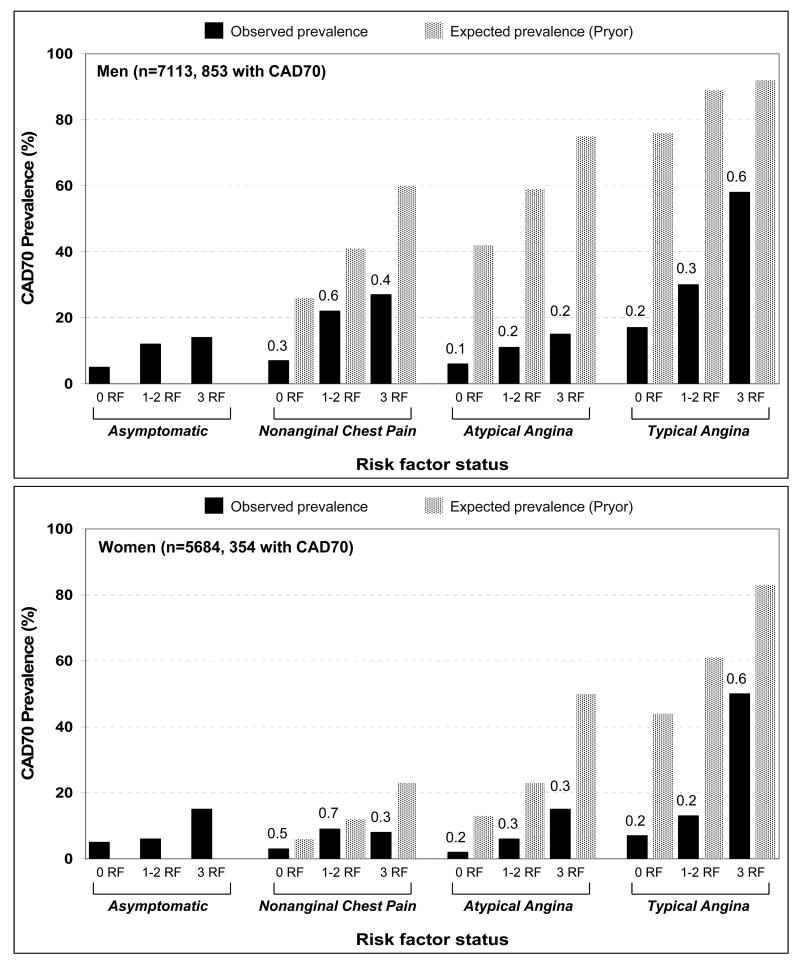
Methods and results: We identified 14048 consecutive patients with suspected CAD who underwent coronary computed tomographic angiography. Angina typicality was recorded with the use of accepted criteria. Pretest likelihoods of CAD with ≥ 50 diameter stenosis (CAD50) and ≥ 70 diameter stenosis (CAD70) were calculated from guideline probabilities. Computed tomographic angiography images were evaluated by ≥ 1 expert reader to determine the presence of CAD50 and CAD70. Typical angina was associated with the highest prevalence of CAD50 (40 in men, 19 in women) and CAD70 (27 men, 11 women) compared with other symptom categories (P<0.001 for all). Observed CAD50 and CAD70 prevalences were substantially lower than those predicted by guideline probabilities in the overall population (18 versus 51 for CAD50, 10 versus 42 for CAD70; P<0.001), driven by pronounced differences in patients with atypical angina (15 versus 47 for CAD50, 7 versus 37 for CAD70) and typical angina (29 versus 86 for CAD50, 19 versus 71 for CAD70). Marked overestimation of disease prevalence by guideline probabilities was found at all participating centers and across all sex and age subgroups.
Conclusion: In this multinational study of patients referred for coronary computed tomographic angiography, determination of pretest likelihood of angiographically significant CAD by the invasive angiography-based guideline probabilities greatly overestimates the actual prevalence of disease.
Conflict of interest statement
Figures
Comment in
-
Right answer, wrong question: on the clinical relevance of the cardiovascular history.Circulation. 2011 Nov 29;124(22):2377-9. doi: 10.1161/CIRCULATIONAHA.111.068718. Circulation. 2011. PMID: 22125189 No abstract available.
-
Coronary artery disease. Age, sex, symptoms, and the prevalence of significant coronary artery disease by coronary computed tomographic angiography.Rev Cardiovasc Med. 2012;13(4):e210-3. doi: 10.3909/ricm0652. Rev Cardiovasc Med. 2012. PMID: 23847794 No abstract available.
References
-
- Gibbons RJ, Abrams J, Chatterjee K, Daley J, Deedwania PC, Douglas JS, Ferguson TB, Jr, Fihn SD, Fraker TD, Jr, Gardin JM, O'Rourke RA, Pasternak RC, Williams SV, Gibbons RJ, Alpert JS, Antman EM, Hiratzka LF, Fuster V, Faxon DP, Gregoratos G, Jacobs AK, Smith SC., Jr ACC/AHA 2002 guideline update for the management of patients with chronic stable angina--summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients With Chronic Stable Angina) Circulation. 2003;107:149–58. - PubMed
-
- Chaitman BR, Bourassa MG, Davis K, Rogers WJ, Tyras DH, Berger R, Kennedy JW, Fisher L, Judkins MP, Mock MB, Killip T. Angiographic prevalence of high-risk coronary artery disease in patient subsets (CASS) Circulation. 1981;64:360–7. - PubMed
-
- Diamond GA, Forrester JS. Analysis of probability as an aid in the clinical diagnosis of coronary-artery disease. N Engl J Med. 1979;300:1350–8. - PubMed
-
- Pryor DB, Harrell FE, Jr, Lee KL, Califf RM, Rosati RA. Estimating the likelihood of significant coronary artery disease. Am J Med. 1983;75:771–80. - PubMed
-
- Pryor DB, Shaw L, McCants CB, Lee KL, Mark DB, Harrell FE, Jr, Muhlbaier LH, Califf RM. Value of the history and physical in identifying patients at increased risk for coronary artery disease. Ann Intern Med. 1993;118:81–90. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
