

Acute infections and venous thromboembolism
- PMID: 22026462
- PMCID: PMC3505369
- DOI: 10.1111/j.1365-2796.2011.02473.x
Acute infections and venous thromboembolism
Abstract
Background: Data on the association between acute infections and venous thromboembolism (VTE) are sparse. We examined whether various hospital-diagnosed infections or infections treated in the community increase the risk of VTE.
Methods: We conducted this population-based case-control study in Northern Denmark (population 1.8 million) using medical databases. We identified all patients with a first hospital-diagnosed VTE during the period 1999-2009 (n = 15 009). For each case, we selected 10 controls from the general population matched for age, gender and county of residence (n = 150 074). We identified all hospital-diagnosed infections and community prescriptions for antibiotics 1 year predating VTE. We used odds ratios from a conditional logistic regression model to estimate incidence rate ratios (IRRs) of VTE within different time intervals of the first year after infection, controlling for confounding.
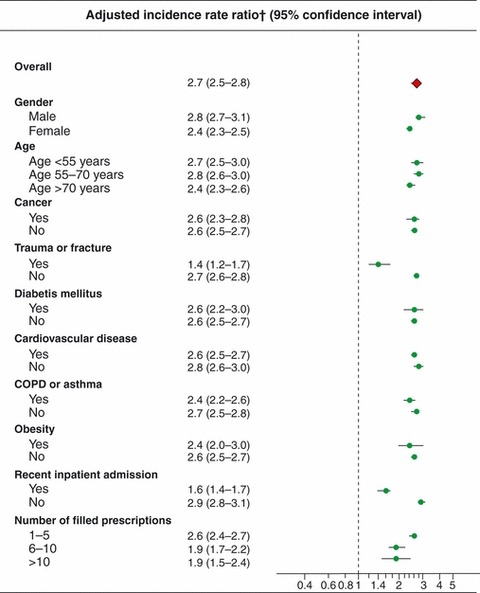
Results: Respiratory tract, urinary tract, skin, intra-abdominal and bacteraemic infections diagnosed in hospital or treated in the community were associated with a greater than equal to twofold increased VTE risk. The association was strongest within the first 2 weeks after infection onset, gradually declining thereafter. Compared with individuals without infection during the year before VTE, the IRR for VTE within the first 3 months after infection was 12.5 (95% confidence interval (CI): 11.3-13.9) for patients with hospital-diagnosed infection and 4.0 (95% CI: 3.8-4.1) for patients treated with antibiotics in the community. Adjustment for VTE risk factors reduced these IRRs to 3.3 (95% CI: 2.9-3.8) and 2.6 (95% CI: 2.5-2.8), respectively. Similar associations were found for unprovoked VTE and for deep venous thrombosis and pulmonary embolism individually.
Conclusions: Infections are a risk factor for VTE.
© 2011 The Association for the Publication of the Journal of Internal Medicine.
Figures
References
-
- Smeeth L, Cook C, Thomas S, Hall AJ, Hubbard R, Vallance P. Risk of deep vein thrombosis and pulmonary embolism after acute infection in a community setting. Lancet. 2006;367:1075–9. - PubMed
-
- Heit JA. The epidemiology of venous thromboembolism in the community: implications for prevention and management. J Thromb Haemost. 2006;21:23–9. - PubMed
-
- Goldhaber SZ. Pulmonary embolism. Lancet. 2004;363:1295–305. - PubMed
-
- Kyrle PA, Eichinger S. Deep vein thrombosis. Lancet. 2005;365:1163–74. - PubMed
-
- Grainge MJ, West J, Card TR. Venous thromboembolism during active disease and remission in inflammatory bowel disease: a cohort study. Lancet. 2010;375:657–63. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
