

Contributions of basal and postprandial hyperglycemia over a wide range of A1C levels before and after treatment intensification in type 2 diabetes
- PMID: 22028279
- PMCID: PMC3220846
- DOI: 10.2337/dc11-0632
Contributions of basal and postprandial hyperglycemia over a wide range of A1C levels before and after treatment intensification in type 2 diabetes
Abstract
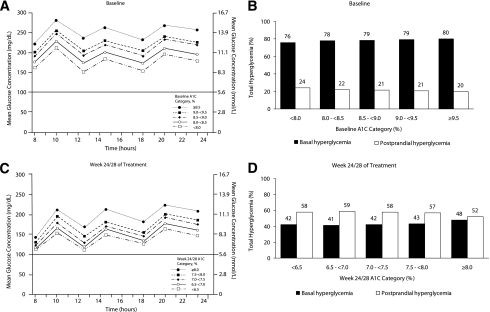
Objective: To determine the relative contributions of basal hyperglycemia (BHG) versus postprandial hyperglycemia (PPHG) before and after treatment intensification in patients with glycated hemoglobin A(1c) (A1C) >7.0% while on prior oral therapy.
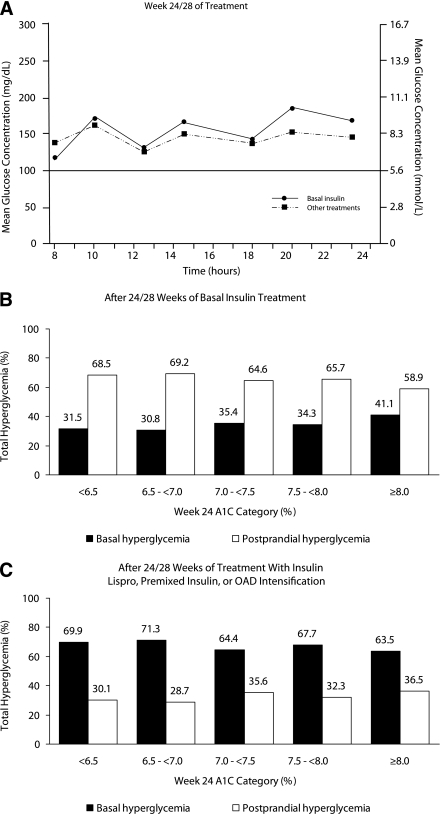
Research design and methods: Self-measured, plasma-referenced glucose profiles and A1C values were evaluated from participants in six studies comparing systematically titrated insulin glargine with an alternative regimen (adding basal, premixed, or prandial insulin, or increasing oral agents). Hyperglycemic exposure (>100 mg/dL [5.6 mmol/L]) as a result of BHG versus PPHG was calculated.
Results: On prior oral therapy, 1,699 participants (mean age 59 years, diabetes duration 9 years) had mean fasting plasma glucose (FPG) of 194 mg/dL (10.8 mmol/L), and mean A1C was 8.7%. BHG contributed an average of 76-80% to hyperglycemia over the observed range of baseline A1C levels. Adding basal insulin for 24 or 28 weeks lowered mean FPG to 117 mg/dL (6.5 mmol/L), A1C to 7.0%, and BHG contribution to 32-41%. Alternative regimens reduced FPG to 146 mg/dL (8.1 mmol/L), A1C to 7.1%, and the contribution of BHG to 64-71%. BHG contributions for patients with A1C averaging 7.6-7.7% were 76% at baseline and 34 and 68% after adding basal insulin or other therapies, respectively.
Conclusions: When A1C is >7.0% despite oral therapy, BHG routinely dominates exposure. Intensified therapy reduces A1C and changes this relationship, but BHG amenable to further intervention still accounts for one-third of total hyperglycemia after basal insulin treatment and two-thirds after alternative methods.
Figures
Comment in
-
Comment on: Riddle et al. Contributions of basal and postprandial hyperglycemia over a wide range of A1C levels before and after treatment intensification in type 2 diabetes. Diabetes Care 2011;34:2508-2514.Diabetes Care. 2012 Jan;35(1):e2; author reply e3. doi: 10.2337/dc11-1857. Diabetes Care. 2012. PMID: 22187445 Free PMC article. No abstract available.
References
-
- Monnier L, Lapinski H, Colette C. Contributions of fasting and postprandial plasma glucose increments to the overall diurnal hyperglycemia of type 2 diabetic patients: variations with increasing levels of HbA(1c). Diabetes Care 2003;26:881–885 - PubMed
-
- Monnier L, Colette C, Dunseath GJ, Owens DR. The loss of postprandial glycemic control precedes stepwise deterioration of fasting with worsening diabetes. Diabetes Care 2007;30:263–269 - PubMed
-
- Peter R, Luzio SD, Dunseath G, Pauvaday V, Mustafa N, Owens DR. Relationship between HbA1c and indices of glucose tolerance derived from a standardized meal test in newly diagnosed treatment naive subjects with Type 2 diabetes. Diabet Med 2006;23:990–995 - PubMed
-
- Peter R, Dunseath G, Luzio SD, Chudleigh R, Choudhury SR, Owens DR. Relative and absolute contributions of postprandial and fasting plasma glucose to daytime hyperglycaemia and HbA(1c) in subjects with Type 2 diabetes. Diabet Med 2009;26:974–980 - PubMed
-
- Kikuchi K, Nezu U, Shirakawa J, et al. Correlations of fasting and postprandial blood glucose increments to the overall diurnal hyperglycemic status in type 2 diabetic patients: variations with levels of HbA1c. Endocr J 2010;57:259–266 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
