

Small-airway obstruction and emphysema in chronic obstructive pulmonary disease
- PMID: 22029978
- PMCID: PMC3238466
- DOI: 10.1056/NEJMoa1106955
Small-airway obstruction and emphysema in chronic obstructive pulmonary disease
Abstract
Background: The major sites of obstruction in chronic obstructive pulmonary disease (COPD) are small airways (<2 mm in diameter). We wanted to determine whether there was a relationship between small-airway obstruction and emphysematous destruction in COPD.
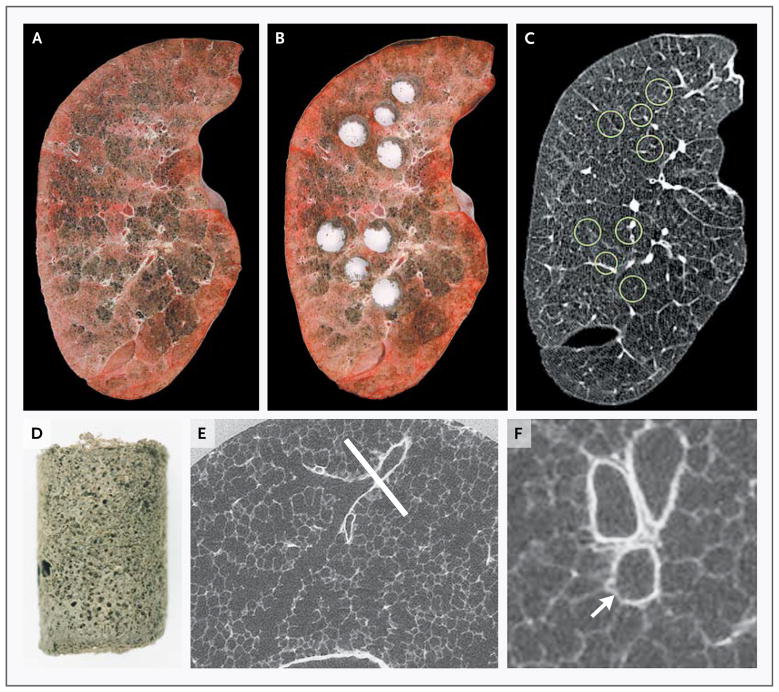
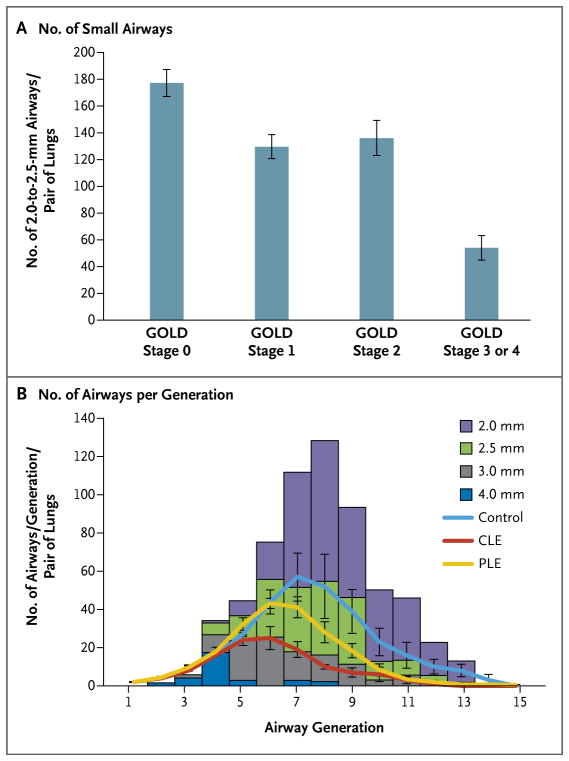
Methods: We used multidetector computed tomography (CT) to compare the number of airways measuring 2.0 to 2.5 mm in 78 patients who had various stages of COPD, as judged by scoring on the Global Initiative for Chronic Obstructive Lung Disease (GOLD) scale, in isolated lungs removed from patients with COPD who underwent lung transplantation, and in donor (control) lungs. MicroCT was used to measure the extent of emphysema (mean linear intercept), the number of terminal bronchioles per milliliter of lung volume, and the minimum diameters and cross-sectional areas of terminal bronchioles.
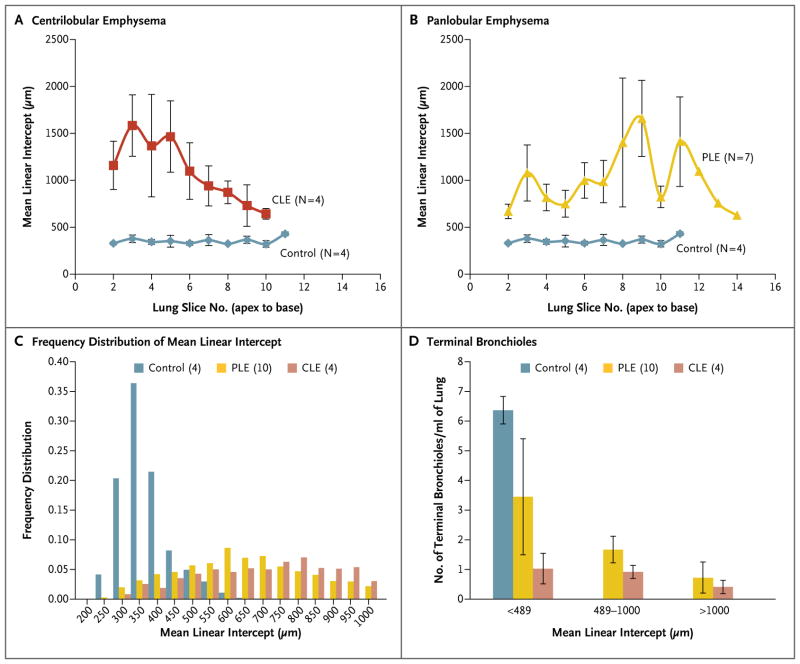
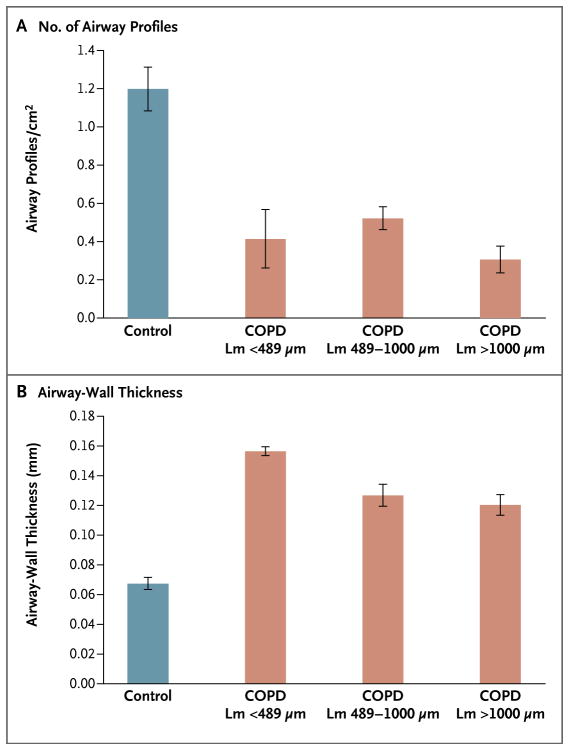
Results: On multidetector CT, in samples from patients with COPD, as compared with control samples, the number of airways measuring 2.0 to 2.5 mm in diameter was reduced in patients with GOLD stage 1 disease (P=0.001), GOLD stage 2 disease (P=0.02), and GOLD stage 3 or 4 disease (P<0.001). MicroCT of isolated samples of lungs removed from patients with GOLD stage 4 disease showed a reduction of 81 to 99.7% in the total cross-sectional area of terminal bronchioles and a reduction of 72 to 89% in the number of terminal bronchioles (P<0.001). A comparison of the number of terminal bronchioles and dimensions at different levels of emphysematous destruction (i.e., an increasing value for the mean linear intercept) showed that the narrowing and loss of terminal bronchioles preceded emphysematous destruction in COPD (P<0.001).
Conclusions: These results show that narrowing and disappearance of small conducting airways before the onset of emphysematous destruction can explain the increased peripheral airway resistance reported in COPD. (Funded by the National Heart, Lung, and Blood Institute and others.).
Figures
Comment in
-
Emphysema--a disease of small airways or lung parenchyma?N Engl J Med. 2011 Oct 27;365(17):1637-9. doi: 10.1056/NEJMe1110635. N Engl J Med. 2011. PMID: 22029986 Free PMC article. No abstract available.
References
-
- Hogg JC, Macklem PT, Thurlbeck WM. Site and nature of airway obstruction in chronic obstructive lung disease. N Engl J Med. 1968;278:1355–60. - PubMed
-
- Van Brabandt H, Cauberghs M, Verbeken E, Moerman P, Lauweryns JM, Van de Woestijne KP. Partitioning of pulmonary impedance in excised human and canine lungs. J Appl Physiol. 1983;55:1733–42. - PubMed
-
- Yanai M, Sekizawa K, Ohrui T, Sasaki H, Takishima T. Site of airway obstruction in pulmonary disease: direct measurement of intrabronchial pressure. J Appl Physiol. 1992;72:1016–23. - PubMed
-
- Pedley TJ, Schroter RC, Sudlow MF. The prediction of pressure drop and variation of resistance within the human bronchial airways. Respir Physiol. 1970;9:387–405. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical