

Diuretic use, increased serum urate levels, and risk of incident gout in a population-based study of adults with hypertension: the Atherosclerosis Risk in Communities cohort study
- PMID: 22031222
- PMCID: PMC3253199
- DOI: 10.1002/art.33315
Diuretic use, increased serum urate levels, and risk of incident gout in a population-based study of adults with hypertension: the Atherosclerosis Risk in Communities cohort study
Abstract
Objective: To quantify the role of diuretic use in gout development in an adult population with hypertension.
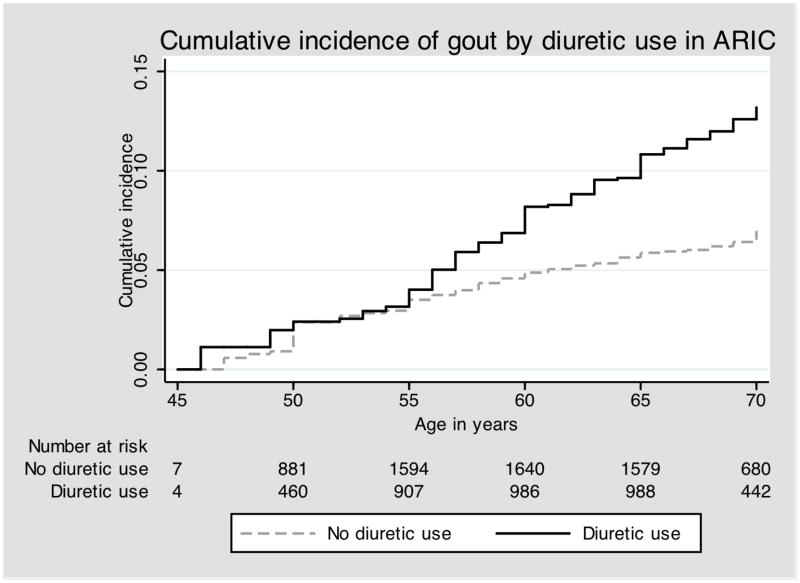
Methods: The Atherosclerosis Risk in Communities study, a prospective population-based cohort from 4 US communities, consisted of 4 visits over a 9-year period. Participants were included in this analysis if they answered a query about gout, were free of gout at baseline, and had hypertension (defined as taking medication to treat hypertension or having blood pressure of ≥140/90 mm Hg). Trained interviewers recorded use of antihypertensive drugs. Incident gout was defined as self-reported onset of gout after baseline. Using a time-dependent Cox proportional hazards model, we estimated hazard ratios (HRs; with 95% confidence intervals [95% CIs]) for incident gout by time-varying diuretic use, both adjusted for confounders and tested for mediation by serum urate level.
Results: There were 5,789 participants with hypertension; 37% were treated with a diuretic. Use of any diuretic (HR 1.48 [95% CI 1.11, 1.98]), a thiazide diuretic (HR 1.44 [95% CI 1.00, 2.10]), or a loop diuretic (HR 2.31 [95% CI 1.36, 3.91]) was associated with incident gout as compared with not using any diuretic, not using a thiazide diuretic, or not using a loop diuretic, respectively. After adjusting for serum urate level, the association between diuretic use and gout was null. Use of antihypertensive medication other than diuretic agents was associated with decreased gout risk (adjusted HR 0.64 [95% CI 0.49, 0.86]) compared to untreated hypertension. The longitudinal change in serum urate levels was 0.72 mg/dl (95% CI 0.57, 0.87) higher in those who began treatment with a diuretic than in those who did not (P<0.001).
Conclusion: Thiazide and loop diuretics were associated with increased gout risk, an association mediated by a change in serum urate levels.
Copyright © 2012 by the American College of Rheumatology.
Conflict of interest statement
Figures
References
-
- Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) JAMA. 2002;288(23):2981–97. - PubMed
-
- Ong HT. The JNC 7 hypertension guidelines. JAMA. 2003;290(10):1312. author reply 1314–5. - PubMed
-
- Staessen J. The determinants and prognostic significance of serum uric acid in elderly patients of the European Working Party on High Blood Pressure in the Elderly trial. Am J Med. 1991;90(3A):50S–54S. - PubMed
-
- Langford HG, Blaufox MD, Borhani NO, Curb JD, Molteni A, Schneider KA, et al. Is thiazide-produced uric acid elevation harmful? Analysis of data from the Hypertension Detection and Follow-up Program. Arch Intern Med. 1987;147(4):645–9. - PubMed
-
- Savage PJ, Pressel SL, Curb JD, Schron EB, Applegate WB, Black HR, et al. Influence of long-term, low-dose, diuretic-based, antihypertensive therapy on glucose, lipid, uric acid, and potassium levels in older men and women with isolated systolic hypertension: The Systolic Hypertension in the Elderly Program. SHEP Cooperative Research Group. Arch Intern Med. 1998;158(7):741–51. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- HHSN-268201100006C/PHS HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- HHSN-268201100010C/PHS HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- HHSN-268201100008C/PHS HHS/United States
- HHSN-268201100009C/PHS HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
- HHSN-268201100011C/PHS HHS/United States
- HHSN-268201100012C/PHS HHS/United States
- HHSN-268201100007C/PHS HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- T32 HL007024/HL/NHLBI NIH HHS/United States
- 5-T32-HL-007024/HL/NHLBI NIH HHS/United States
- HHSN-268201100005C/PHS HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
