

Plasma cells and the chronic nonsuppurative destructive cholangitis of primary biliary cirrhosis
- PMID: 22031474
- PMCID: PMC3272098
- DOI: 10.1002/hep.24757
Plasma cells and the chronic nonsuppurative destructive cholangitis of primary biliary cirrhosis
Abstract
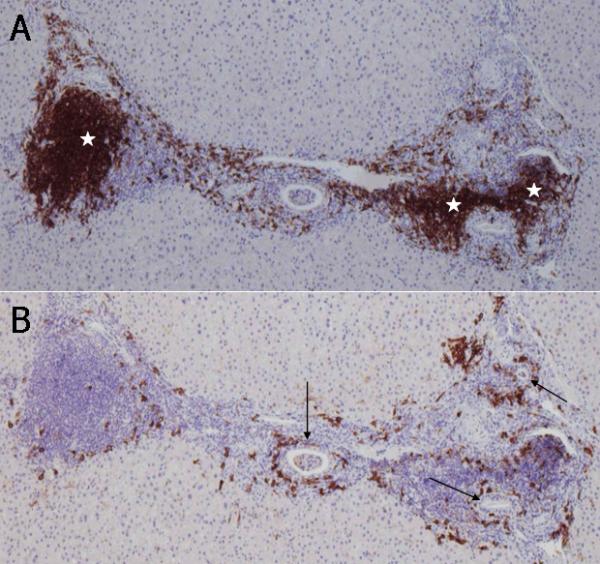
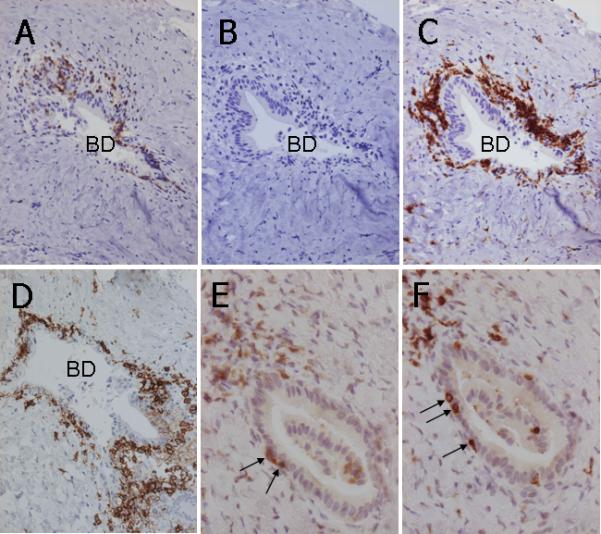
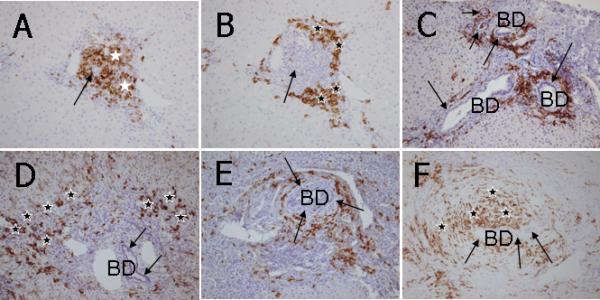
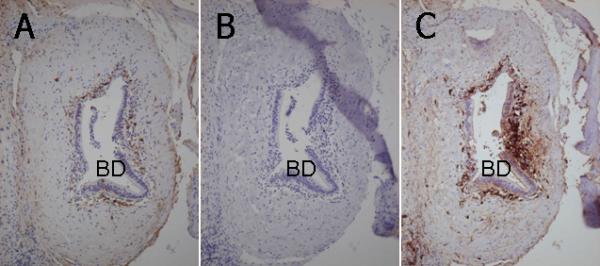
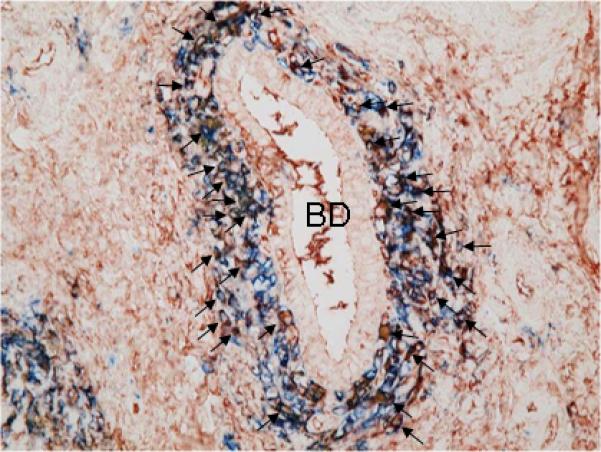
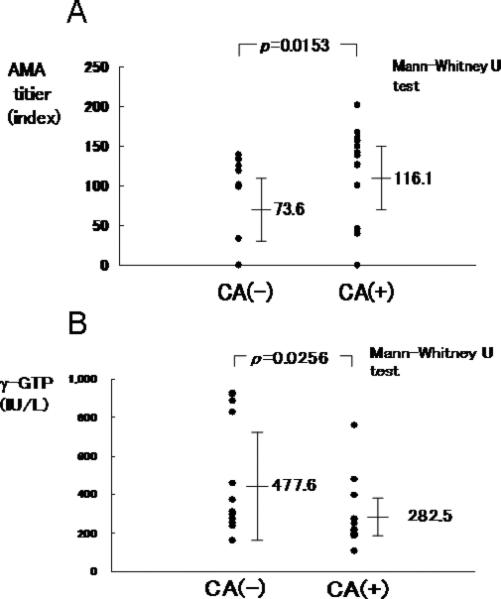
There has been increased interest in the role of B cells in the pathogenesis of primary biliary cirrhosis (PBC). Although the vast majority of patients with this disease have anti-mitochondrial antibodies, there is no correlation of anti-mitochondrial antibody titer and/or presence with disease severity. Furthermore, in murine models of PBC, it has been suggested that depletion of B cells may exacerbate biliary pathology. To address this issue, we focused on a detailed phenotypic characterization of mononuclear cell infiltrates surrounding the intrahepatic bile ducts of patients with PBC, primary sclerosing cholangitis, autoimmune hepatitis, chronic hepatitis C, and graft-versus-host disease, including CD3, CD4, CD8, CD20, CD38, and immunoglobulin classes, as well as double immunohistochemical staining for CD38 and IgM. Interestingly, CD20 B lymphocytes, which are a precursor of plasma cells, were found in scattered locations or occasionally forming follicle-like aggregations but were not noted at the proximal location of chronic nonsuppurative destructive cholangitis. In contrast, there was a unique and distinct coronal arrangement of CD38 cells around the intrahepatic ducts in PBC but not controls; the majority of such cells were considered plasma cells based on their expression of intracellular immunoglobulins, including IgM and IgG, but not IgA. Patients with PBC who manifest this unique coronal arrangement were those with significantly higher titers of anti-mitochondrial antibodies.
Conclusion: These data collectively suggest a role for plasma cells in the specific destruction of intrahepatic bile ducts in PBC and confirm the increasing interest in plasma cells and autoimmunity.
Copyright © 2011 American Association for the Study of Liver Diseases.
Figures
References
-
- Kaplan MM, Gershwin ME. Primary biliary cirrhosis. N Engl J Med. 2005;353:1261–1273. - PubMed
-
- Gershwin ME, Mackay IR, Sturgess A, Coppel RL. Identification and specificity of a cDNA encoding the 70 kd mitochondrial antigen recognized in primary biliary cirrhosis. J Immunol. 1987;138:3525–3531. - PubMed
-
- Moritoki Y, Zhang W, Tsuneyama K, Yoshida K, Wakabayashi K, Yang GX, Bowlus C, et al. B cells suppress the inflammatory response in a mouse model of primary biliary cirrhosis. Gastroenterology. 2009;136:1037–1047. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous