

Can anti-cyclic citrullinated peptide antibody-negative RA be subdivided into clinical subphenotypes?
- PMID: 22032620
- PMCID: PMC3308115
- DOI: 10.1186/ar3505
Can anti-cyclic citrullinated peptide antibody-negative RA be subdivided into clinical subphenotypes?
Abstract
Introduction: Studies investigating genetic risk factors for susceptibility to rheumatoid arthritis (RA) studied anti-citrullinated peptide antibody (CCP)-positive RA more frequently than anti-CCP-negative RA. One of the reasons for this is the perception that anti-CCP-negative RA may include patients that fulfilled criteria for RA but belong to a wide range of diagnoses. We aimed to evaluate the validity of this notion and explored whether clinical subphenotypes can be discerned within anti-CCP-negative RA.
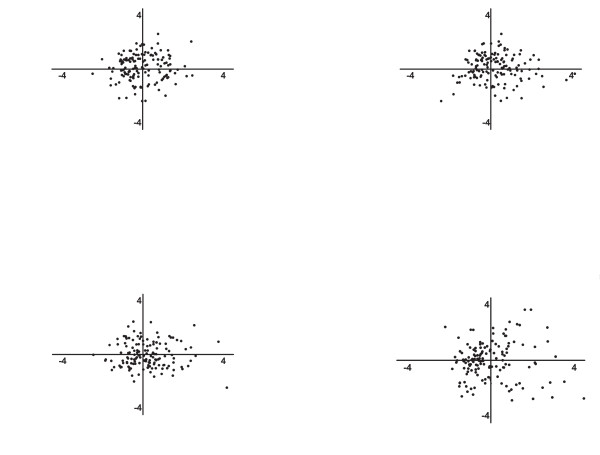
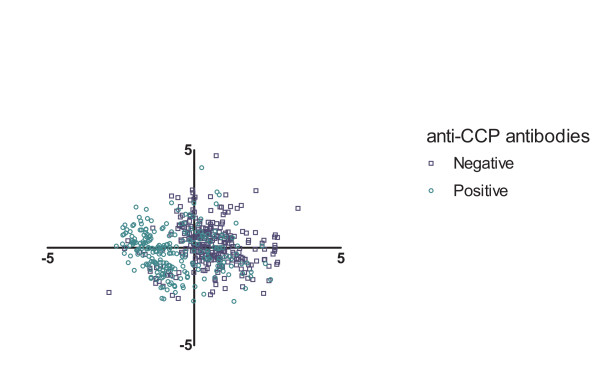
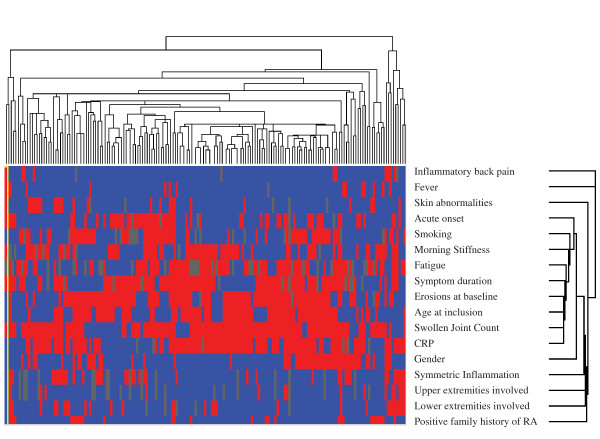
Methods: The 318 patients with anti-CCP-negative RA (1987 ACR criteria), included in the Leiden Early Arthritis Clinic between 1993 and 2006, were studied for baseline characteristics and radiologic progression data during a mean follow-up of 5 years. Grouping was studied both at variable and patient levels. Principal components analysis and partial least-squares regression were applied to study for clustering of variables. A cluster analysis was performed to look for clustering of patients.
Results: The simultaneous presence of patient characteristics at disease presentation was observed for several groups; however, the three largest groups of patients' characteristics explained only 26.5% of the total variance. Plotting the contribution of each patient to these three groups did not reveal clustering of patients. Comparable observations were made when data on progression of joint destruction were studied in relation to baseline clinical data. A cluster analysis, evaluating whether patients resemble each other, revealed no grouping of patients. Altogether, no clinically distinguishable subphenotypes were observed.
Conclusions: The current data provide evidence that, for risk-factor studies, anti-CCP-negative RA patients can be studied as one group.
Figures
References
-
- Pratt AG, Charles PJ, Chowdhury M, Wilson G, Venables PJ, Isaacs JD. Serotyping for an extended anti-citrullinated peptide autoantibody panel does not add value to CCP2 testing for diagnosing RA in an early undifferentiated arthritis cohort. Ann Rheum Dis. 2011;70:2056–2058. doi: 10.1136/ard.2010.148197. - DOI - PubMed
-
- Padyukov L, Seielstad M, Ong RT, Ding B, Ronnelid J, Seddighzadeh M, Alfredsson L, Klareskog L. A genome-wide association study suggests contrasting associations in ACPA-positive versus ACPA-negative rheumatoid arthritis. Ann Rheum Dis. 2011;70:259–265. doi: 10.1136/ard.2009.126821. - DOI - PMC - PubMed
-
- van Oosterhout M, Bajema I, Levarht EW, Toes RE, Huizinga TW, van Laar JM. Differences in synovial tissue infiltrates between anti-cyclic citrullinated peptide-positive rheumatoid arthritis and anti-cyclic citrullinated peptide-negative rheumatoid arthritis. Arthritis Rheum. 2008;58:53–60. doi: 10.1002/art.23148. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
