

Neurobiological consequences of traumatic brain injury
- PMID: 22033563
- PMCID: PMC3182015
- DOI: 10.31887/DCNS.2011.13.2/tmcallister
Neurobiological consequences of traumatic brain injury
Abstract
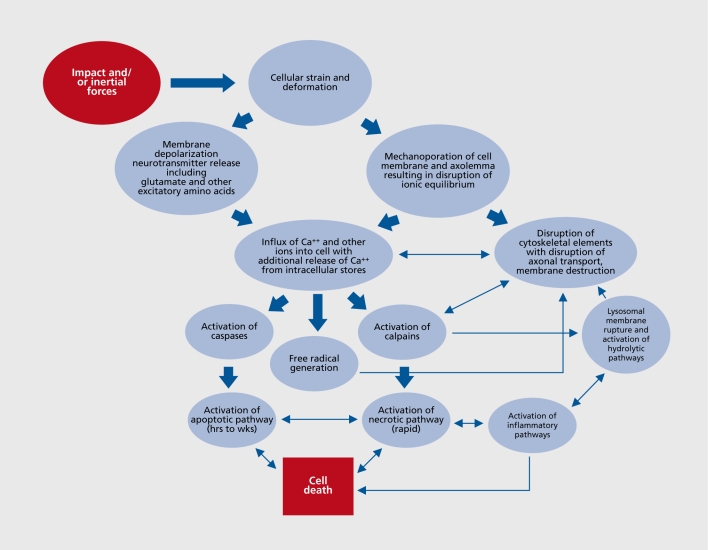
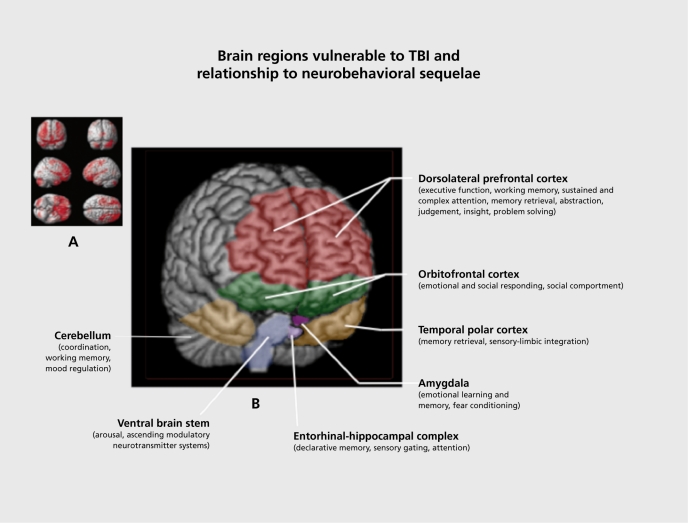
Traumatic brain injury (TBI) is a worldwide public health problem typically caused by contact and inertial forces acting on the brain. Recent attention has also focused on the mechanisms of injury associated with exposure to blast events or explosions. Advances in the understanding of the neuropathophysiology of TBI suggest that these forces initiate an elaborate and complex array of cellular and subcellular events related to alterations in Ca(++) homeostasis and signaling. Furthermore, there is a fairly predictable profile of brain regions that are impacted by neurotrauma and the related events. This profile of brain damage accurately predicts the acute and chronic sequelae that TBI survivors suffer from, although there is enough variation to suggest that individual differences such as genetic polymorphisms and factors governing resiliency play a role in modulating outcome. This paper reviews our current understanding of the neuropathophysiology of TBI and how this relates to the common clinical presentation of neurobehavioral difficulties seen after an injury.
El daño cerebral traumático (DCT) es un problema de salud pública mundial causado característicamente por fuerzas de contacto o de inercia que actúan sobre el cerebro. La preocupación reciente se ha centrado en los mecanismos de daño asociado con la exposición al efecto de ráfagas o explosiones. Los avances en la comprensión de la neurofisiopatologáa del DCT sugieren que estas fuerzas inician y producen una serie compleja de acontecimientos celulares y subcelulares relacionados con alteraciones en la homeostasis y mecanismos de señales del Ca++. Además, hay un perfil bastante predecible de regiones cerebrales que son afectadas por el neurotrauma y los acontecimientos relacionados. Este perfil de daño cerebral predice con precisión las secuelas agudas y crónicas que sufren los supervivientes de un DCT, aunque existe bastante variación que sugiere que las diferencias individuales - como los polimorfismos genéticos y los factores que regulan la resiliencia - tienen un papel en la modulación de los resultados. Este artículo revisa la comprensión actual de la neurofisiopatología del DCT y cómo se relaciona ésta con la presentación clínica habitual de las dificultades neuroconductuales que se observan después de una lesión.
La lésion cérébrale traumatique (LCT), problème de santé publique mondial, est provoquée par un contact et des forces d'inertie agissant sur le cerveau. Récemment, l'intérêt s'est porté aussi sur les mécanismes des lésions associées aux explosions ou aux phénomènes de souffle. Les avancées dans la compréhension de la neurophysiopathologie de la LCT laissent supposer que ces forces sont à l'origine d'une série élaborée et complexe d'événements cellulaires et sous-cellulaires liés aux altérations de l'homéostasie et du signal calciques. De plus, le profil des régions cérébrales touchées par les neurotraumatismes et les événements liés est assez prévisible. Le profil de la lésion cérébrale prédit précisément les séquelles aiguës et chroniques des survivants aux LCT, les variations étant néanmoins suffisantes pour suggérer que des différences individuelles (polymorphismes génétiques et facteurs de resilience) jouent un rôle dans la modulation de l'évolution. Cet article fait une mise au point sur notre compréhension actuelle de la neurophysiopathologie de la LCT et sur la façon dont on peut la rattacher aux problèmes neurocomportementaux observés après une lésion.
Keywords: neurobehavior; neuropsychiatry of TBI; neurotrauma; traumatic brain injury.
Figures
References
-
- Kay T., Harrington DE., Adams R., et al. Definition of mild traumatic brain injury. J Head Trauma Rehabil. 1993;8:86–87.
-
- Thurman D., Alverson C., Browne D., et al. Traumatic Brain Injury in the United States: A Report to Congress. Centers for Disease Control and Prevention. 1999
-
- Carroll LJ., Cassidy JD., Peloso PM., et al. Prognosis for mild traumatic brain injury: Results of the who collaborating centre task force on mild traumatic brain injury. J Rehabil Med. 2004;(43 suppl):84–105. - PubMed
-
- Menon D., Schwab K., Wright D., Maas A. Position statement: definition of traumatic brain injury. Arch Phys Med Rehabil. 2010;91:1637–1640. - PubMed
-
- Iverson GL., Lange RT. Examination of “postconcussion-like” symptoms in a healthy sample. Appl Neuropsychol. 2003;10:137–144. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials