

Endovascular treatment of cavernous sinus aneurysms
- PMID: 22033713
- PMCID: PMC7964783
- DOI: 10.3174/ajnr.A2759
Endovascular treatment of cavernous sinus aneurysms
Abstract
Background and purpose: Aneurysms of the cavernous segment of the internal carotid artery generally exhibit a benign clinical course, with mass effect on cranial nerves. Rupture generally leads to carotid cavernous fistula and, rarely, to subarachnoid hemorrhage. In this study we report results of treatment in 85 patients with 86 cavernous sinus aneurysms.
Materials and methods: In a 15-year period, 85 patients with 86 cavernous sinus aneurysms were treated. There were 77 women (91%) and 8 men, with a mean age of 55.5 years (range 26-78 years). Presentation was cranial neuropathy in 56, carotid cavernous fistula in 8, and subarachnoid hemorrhage in 1 patient. Twenty-one aneurysms were asymptomatic. Treatment was selective coiling in 31 aneurysms and carotid artery occlusion in 55 aneurysms, 5 after bypass surgery.
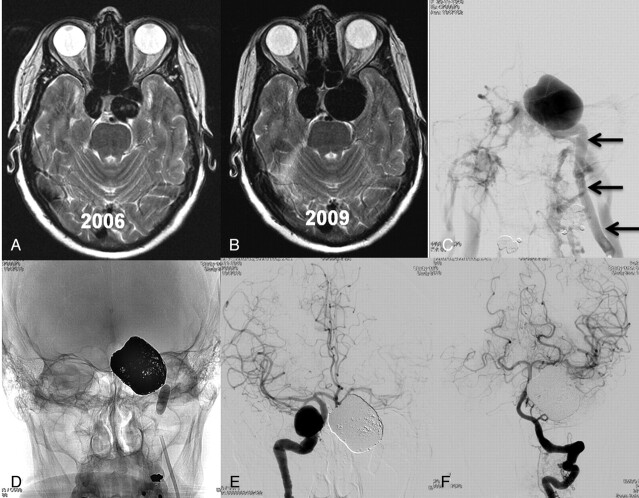
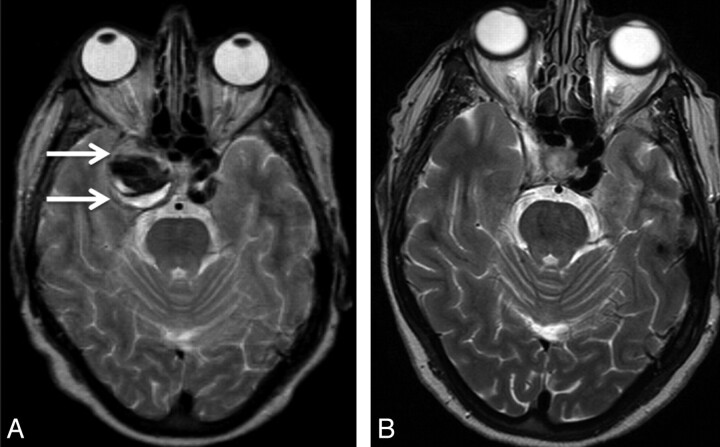
Results: All 8 cavernous sinus fistulas were closed with coils. There were no complications of coiling and 1 patient had a permanent neurologic complication after carotid artery occlusion (morbidity 1.2%; 95% confidence interval, 0.01 to 6.9%). Clinical and MR imaging follow-up ranged from 3 months to 12 years. In 52 of 56 (93%) patients presenting with symptoms of mass effect, symptoms either were cured (n = 23) or improved (n = 29). All aneurysms were thrombosed after carotid artery occlusion and at latest MR imaging, 34 of 50 aneurysms (68%) were substantially decreased in size or completely obliterated.
Conclusions: In this series, for patients with cavernous sinus aneurysms, a treatment strategy including selective coiling and carotid artery occlusion was safe and effective. Most symptomatic patients (93%) were improved or cured, and most aneurysms (68%) shrank on follow-up.
Figures
Comment in
-
Cavernous sinus segment internal carotid artery aneurysms: whether and how to treat.AJNR Am J Neuroradiol. 2012 Feb;33(2):327-8. doi: 10.3174/ajnr.A3031. Epub 2012 Feb 2. AJNR Am J Neuroradiol. 2012. PMID: 22300929 Free PMC article. No abstract available.
Similar articles
-
Endovascular coiling versus parent artery occlusion for treatment of cavernous carotid aneurysms: a meta-analysis.J Neurointerv Surg. 2015 Apr;7(4):250-5. doi: 10.1136/neurintsurg-2014-011102. Epub 2014 Mar 21. J Neurointerv Surg. 2015. PMID: 24658655
-
Ruptured cavernous sinus aneurysms causing carotid cavernous fistula: incidence, clinical presentation, treatment, and outcome.AJNR Am J Neuroradiol. 2006 Jan;27(1):185-9. AJNR Am J Neuroradiol. 2006. PMID: 16418380 Free PMC article.
-
Unruptured large and giant carotid artery aneurysms presenting with cranial nerve palsy: comparison of clinical recovery after selective aneurysm coiling and therapeutic carotid artery occlusion.AJNR Am J Neuroradiol. 2008 May;29(5):997-1002. doi: 10.3174/ajnr.A1023. Epub 2008 Feb 22. AJNR Am J Neuroradiol. 2008. PMID: 18296545 Free PMC article. Clinical Trial.
-
Cavernous internal carotid artery aneurysms treated with electrolytically detachable coils.J Neuroophthalmol. 1997 Dec;17(4):231-9. J Neuroophthalmol. 1997. PMID: 9427173
-
Endovascular treatment of aneurysms in the cavernous sinus: a systematic review on balloon occlusion of the parent vessel and embolization with coils.Stroke. 2002 Jan;33(1):313-8. doi: 10.1161/hs0102.101479. Stroke. 2002. PMID: 11779933
Cited by
-
Flow diverters for unruptured internal carotid artery aneurysms: dangerous and not yet an alternative for conventional endovascular techniques.AJNR Am J Neuroradiol. 2013 Jan;34(1):3-4. doi: 10.3174/ajnr.A3317. Epub 2012 Aug 23. AJNR Am J Neuroradiol. 2013. PMID: 22918425 Free PMC article. No abstract available.
-
Aneurysm Study of Pipeline in an Observational Registry (ASPIRe).Interv Neurol. 2016 Jun;5(1-2):89-99. doi: 10.1159/000446503. Epub 2016 May 26. Interv Neurol. 2016. PMID: 27610126 Free PMC article.
-
Is flow diversion the death of cerebral bypass and coiling/stent-assisted coiling for giant cavernous aneurysms? A critical review on comparative outcomes and ongoing clinical trials.Neurosurg Rev. 2013 Oct;36(4):505-11; discussion 511-2. doi: 10.1007/s10143-013-0459-9. Epub 2013 Apr 18. Neurosurg Rev. 2013. PMID: 23595654 Review.
-
Treatment of cavernous sinus aneurysms with flow diversion: results in 44 patients.AJNR Am J Neuroradiol. 2014 May;35(5):948-51. doi: 10.3174/ajnr.A3826. Epub 2013 Dec 19. AJNR Am J Neuroradiol. 2014. PMID: 24356675 Free PMC article.
-
Aneurysmal Subarachnoid Hemorrhage.J Neurosurg Anesthesiol. 2015 Jul;27(3):222-40. doi: 10.1097/ANA.0000000000000130. J Neurosurg Anesthesiol. 2015. PMID: 25272066 Free PMC article. Review.
References
-
- Linskey ME, Sekhar LN, Hirsch WL, et al. . Aneurysms of the intracavernous carotid artery: natural history and indications for treatment. Neurosurgery 1990; 26: 933–37 - PubMed
-
- Kupersmith MJ, Hurst R, Berenstein A, et al. . The benign course of cavernous carotid artery aneurysms. J Neurosurg 1992; 77: 690–93 - PubMed
-
- Kupersmith MJ, Stiebel-Kalish H, Huna-Baron R, et al. . Cavernous carotid aneurysms rarely cause subarachnoid hemorrhage or major neurologic morbidity. J Stroke Cerebrovasc Dis 2002; 11: 9–14 - PubMed
-
- Stiebel-Kalish H, Kalish Y, Bar-On RH, et al. . Presentation, natural history, and management of carotid cavernous aneurysms. Neurosurgery 2005; 57: 850–57 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical