

Cervical and lumbar spinal arthroplasty: clinical review
- PMID: 22033716
- PMCID: PMC7964765
- DOI: 10.3174/ajnr.A2758
Cervical and lumbar spinal arthroplasty: clinical review
Abstract
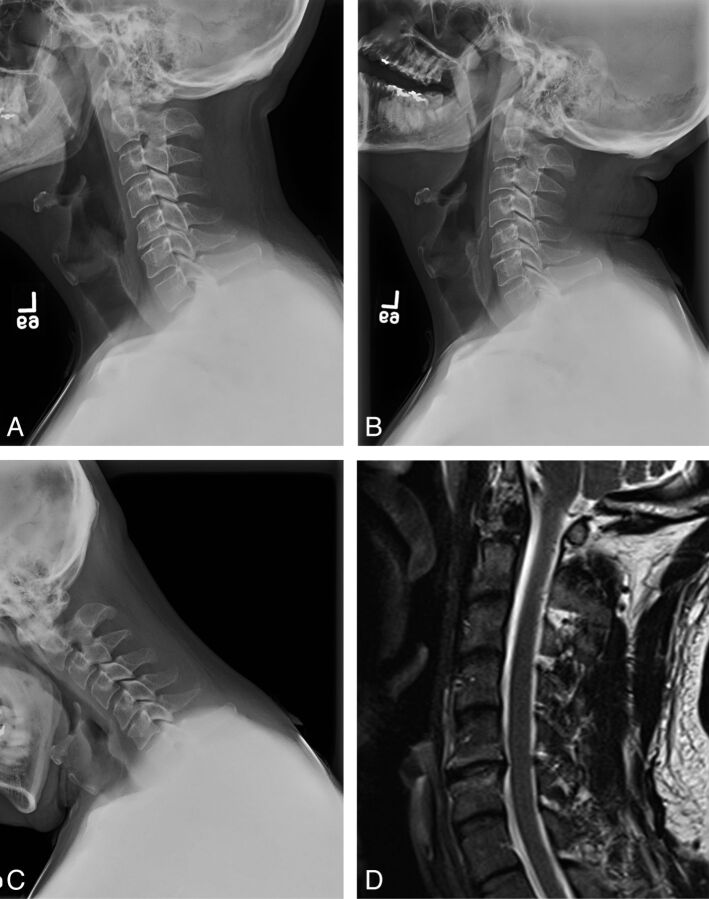
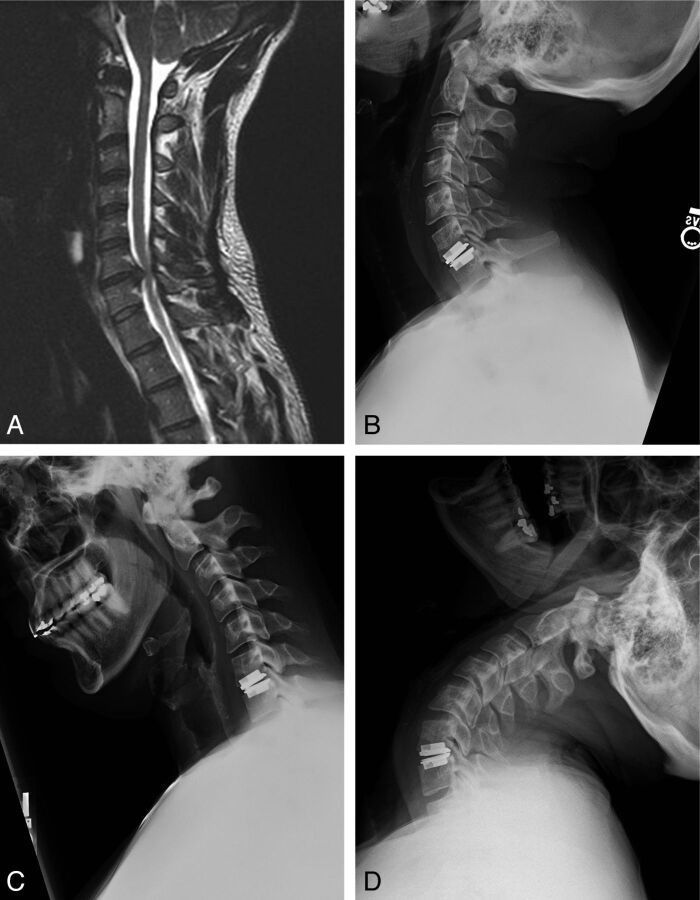
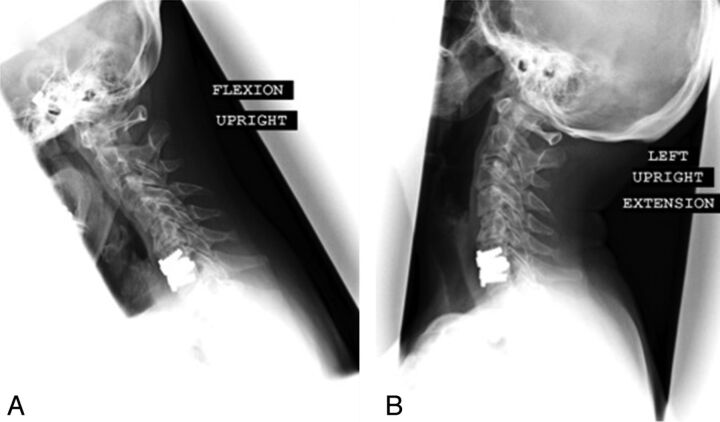
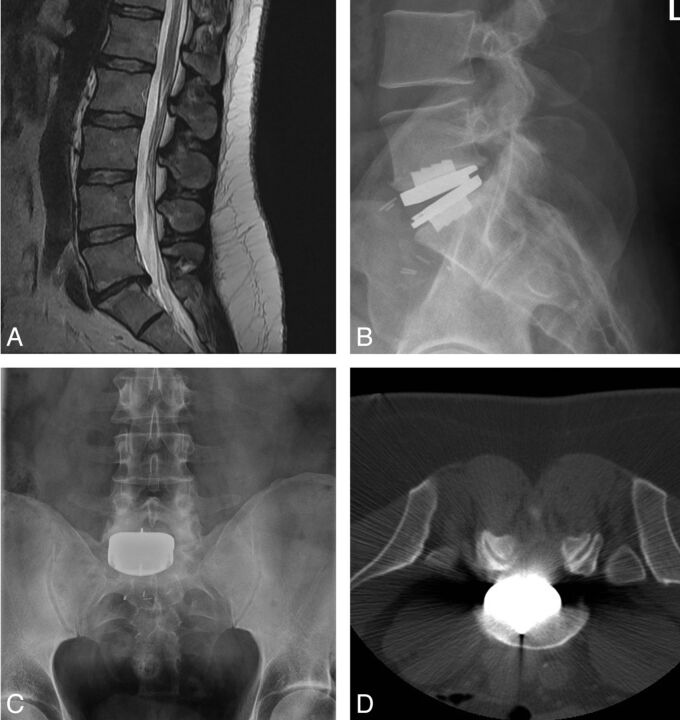
In contrast to cervical and lumbar fusion procedures, the principal aim of disk arthroplasty is to recapitulate the normal kinematics and biomechanics of the spinal segment affected. Following decompression of the neural elements, disk arthroplasty allows restoration of disk height and maintenance of spinal alignment. Based on clinical observations and biomechanical testing, the anticipated advantage of arthroplasty over standard arthrodesis techniques has been a proposed reduction in the development of symptomatic ALD. In this review of cervical and lumbar disk arthroplasty, we highlight the clinical results and experience with standard fusion techniques, incidence of ALD in the population of patients with surgical fusion, and indications for arthroplasty, as well as the biomechanical and clinical outcomes following arthroplasty. In addition, we introduce the devices currently available and provide a critical appraisal of the clinical evidence regarding arthroplasty procedures.
Figures
Similar articles
-
Review of long-term outcomes of disc arthroplasty for symptomatic single level cervical degenerative disc disease.Expert Rev Med Devices. 2018 Mar;15(3):205-217. doi: 10.1080/17434440.2018.1433533. Epub 2018 Feb 5. Expert Rev Med Devices. 2018. PMID: 29378457
-
Cervical Disc Arthroplasty: Review and Update for Radiologists.Semin Roentgenol. 2019 Apr;54(2):113-123. doi: 10.1053/j.ro.2018.06.001. Epub 2018 Jun 6. Semin Roentgenol. 2019. PMID: 31128736 Review. No abstract available.
-
Comparison of Different Hybrid Techniques for the Treatment of Multilevel Cervical Degenerative Disc Disease-Analysis of Prospectively Collected Clinical, Radiologic, and Psychological Parameters.World Neurosurg. 2020 Aug;140:e112-e120. doi: 10.1016/j.wneu.2020.04.182. Epub 2020 May 1. World Neurosurg. 2020. PMID: 32371075
-
Lumbar Disk Arthroplasty for Degenerative Disk Disease: Literature Review.World Neurosurg. 2018 Jan;109:188-196. doi: 10.1016/j.wneu.2017.09.153. Epub 2017 Oct 4. World Neurosurg. 2018. PMID: 28987839 Review.
-
Cervical disk arthroplasty versus ACDF for preoperative reducible kyphosis.Orthopedics. 2013 Jul;36(7):e958-65. doi: 10.3928/01477447-20130624-29. Orthopedics. 2013. PMID: 23823056 Clinical Trial.
Cited by
-
Preliminary exploration of the biomechanical properties of three novel cervical porous fusion cages using a finite element study.BMC Musculoskelet Disord. 2023 Nov 10;24(1):876. doi: 10.1186/s12891-023-06999-2. BMC Musculoskelet Disord. 2023. PMID: 37950220 Free PMC article.
-
Spinal motion preservation surgery: indications and applications.Eur J Orthop Surg Traumatol. 2018 Apr;28(3):335-342. doi: 10.1007/s00590-017-2052-3. Epub 2017 Oct 6. Eur J Orthop Surg Traumatol. 2018. PMID: 28986691 Review.
-
Adhesive Hydrogel Building Blocks to Reconstruct Complex Cartilage Tissues.ACS Biomater Sci Eng. 2023 Apr 10;9(4):1952-1960. doi: 10.1021/acsbiomaterials.2c01438. Epub 2023 Mar 7. ACS Biomater Sci Eng. 2023. PMID: 36881710 Free PMC article.
-
We Need to Talk about Lumbar Total Disc Replacement.Int J Spine Surg. 2018 Aug 3;12(2):201-240. doi: 10.14444/5029. eCollection 2018 Apr. Int J Spine Surg. 2018. PMID: 30276080 Free PMC article.
-
Lumbar disc replacement surgery-successes and obstacles to widespread adoption.Curr Rev Musculoskelet Med. 2017 Jun;10(2):153-159. doi: 10.1007/s12178-017-9397-4. Curr Rev Musculoskelet Med. 2017. PMID: 28324327 Free PMC article. Review.
References
-
- Cloward RB. Vertebral body fusion for ruptured cervical discs. Am J Surg 1959; 98: 722– 27 - PubMed
-
- Bailey RW, Badgley CE. Stabilization of the cervical spine by anterior fusion. J Bone Joint Surg Am 1960; 42-A: 565– 94 - PubMed
-
- Robinson RA. The problem of neck pain: its alleviation by anterior removal of intervertebral disc with interbody fusion in the cervical spine. J Med Assoc State Ala 1963; 33: 1– 14 - PubMed
-
- Smith GW, Robinson RA. The treatment of certain cervical-spine disorders by anterior removal of the intervertebral disc and interbody fusion. J Bone Joint Surg Am 1958; 40-A: 607– 24 - PubMed
-
- Chiles BW, 3rd, Leonard MA, Choudhri HF, et al. . Cervical spondylotic myelopathy: patterns of neurological deficit and recovery after anterior cervical decompression. Neurosurgery 1999; 44: 762– 69, discussion 769–70 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical