

Cardiac magnetic resonance imaging and its electrocardiographs (ECG): tips and tricks
- PMID: 22033762
- PMCID: PMC3476721
- DOI: 10.1007/s10554-011-9957-4
Cardiac magnetic resonance imaging and its electrocardiographs (ECG): tips and tricks
Abstract
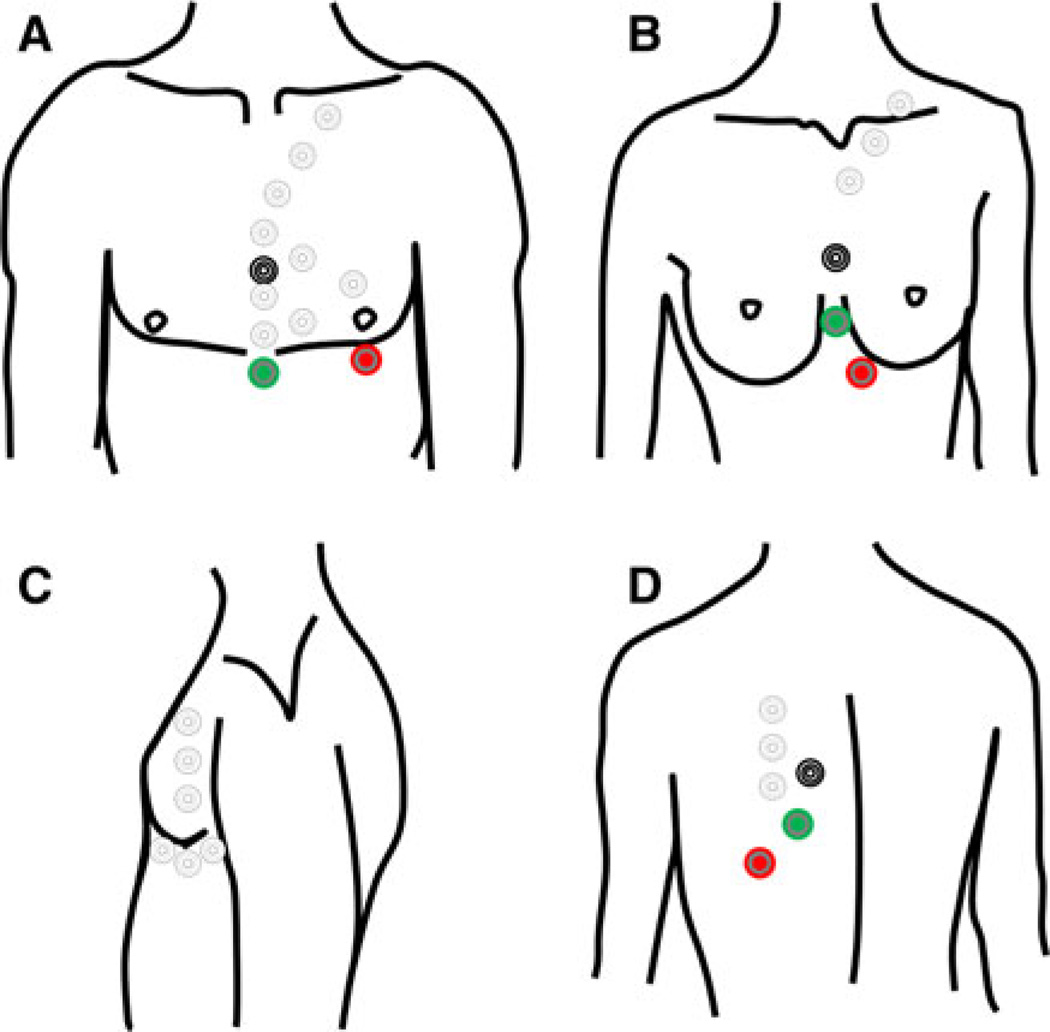
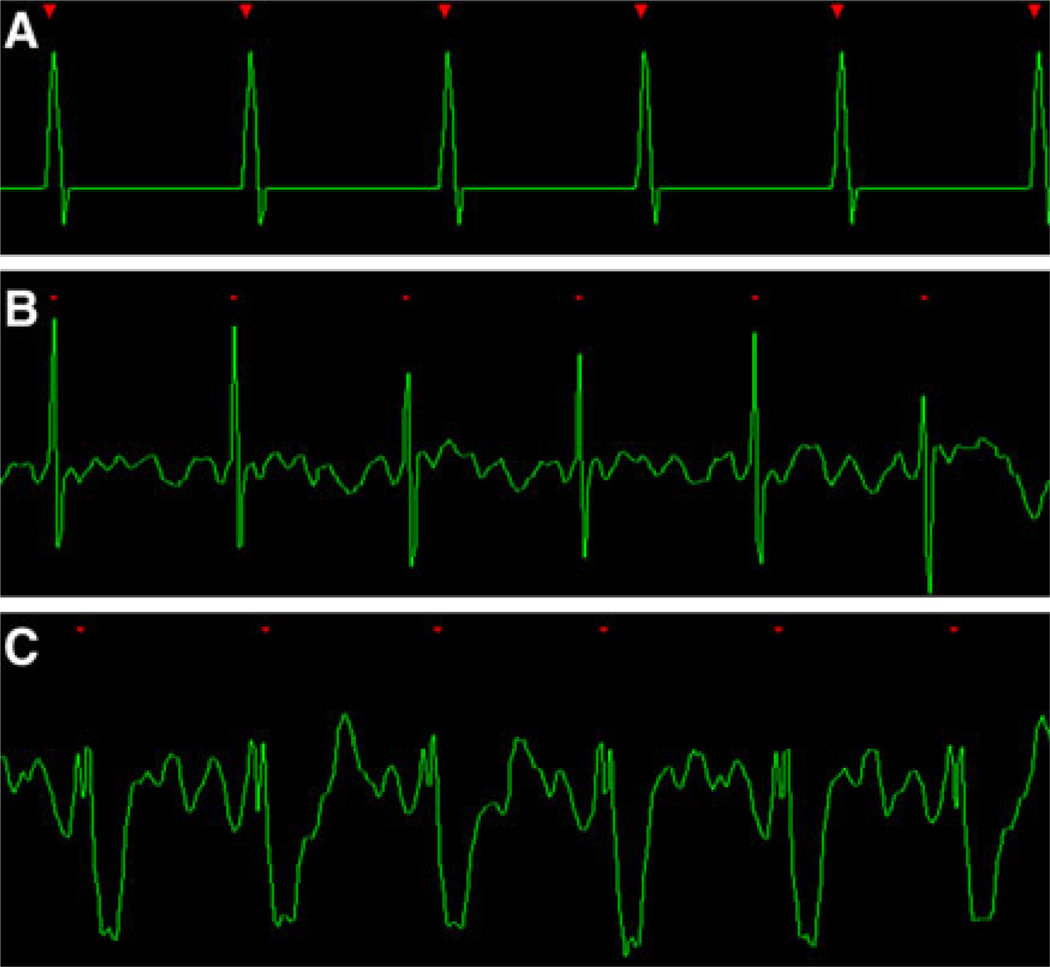
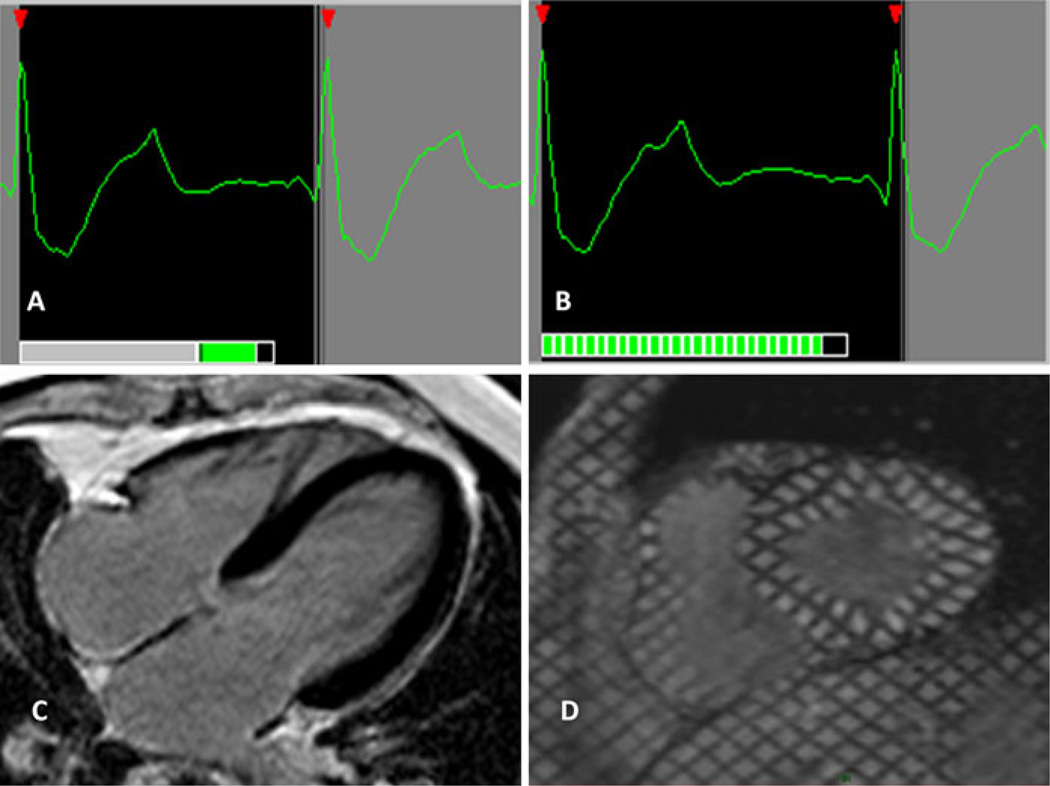
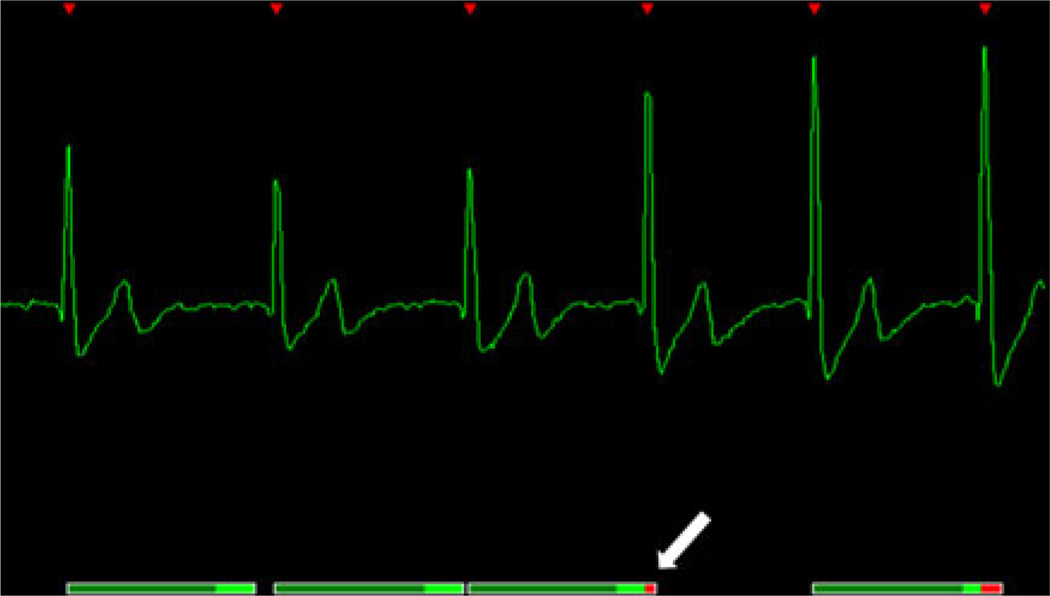
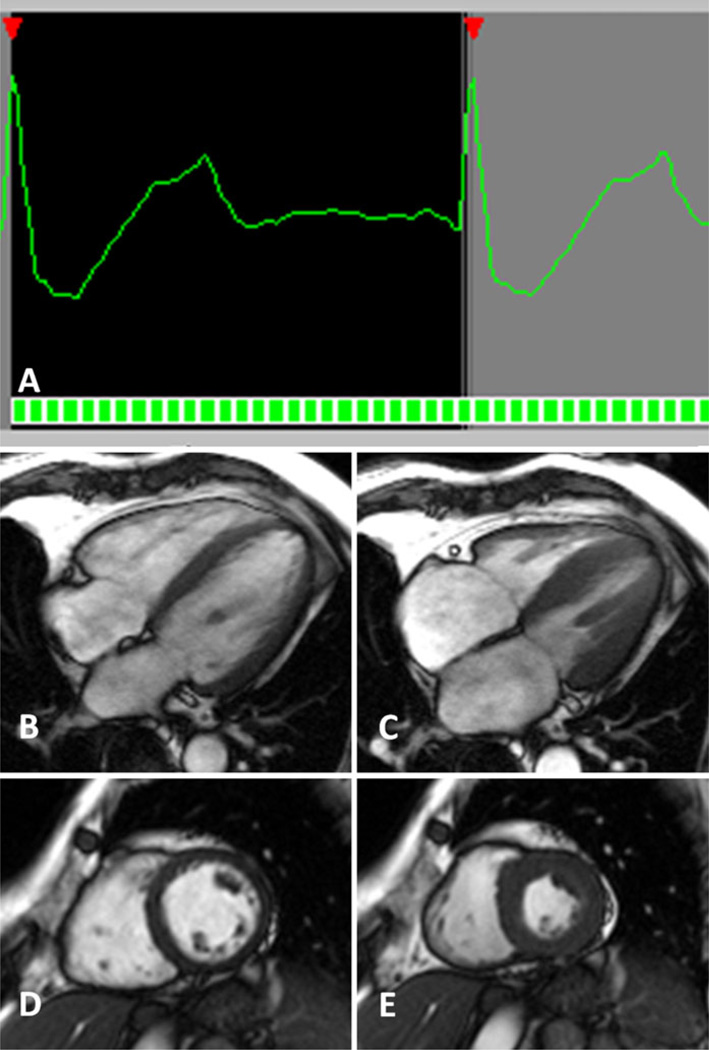
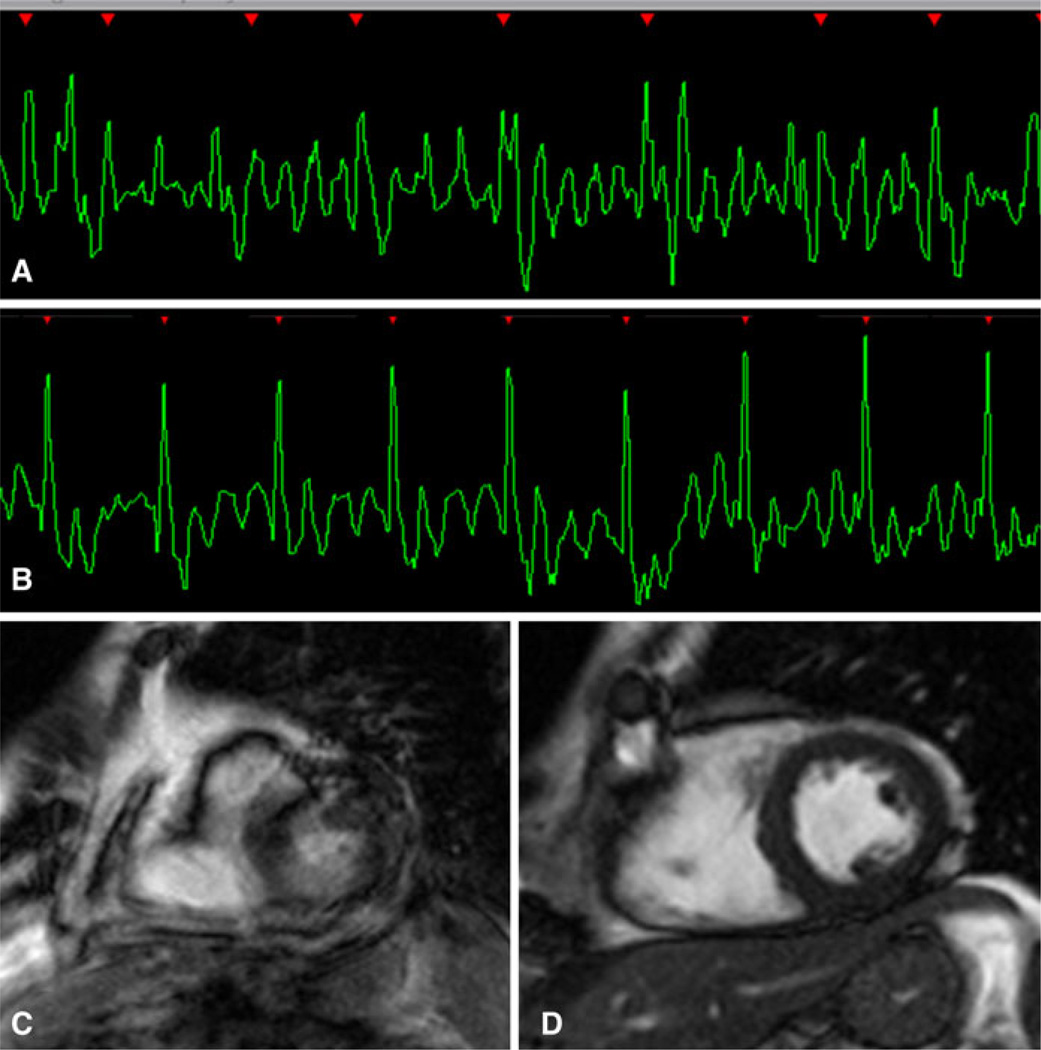
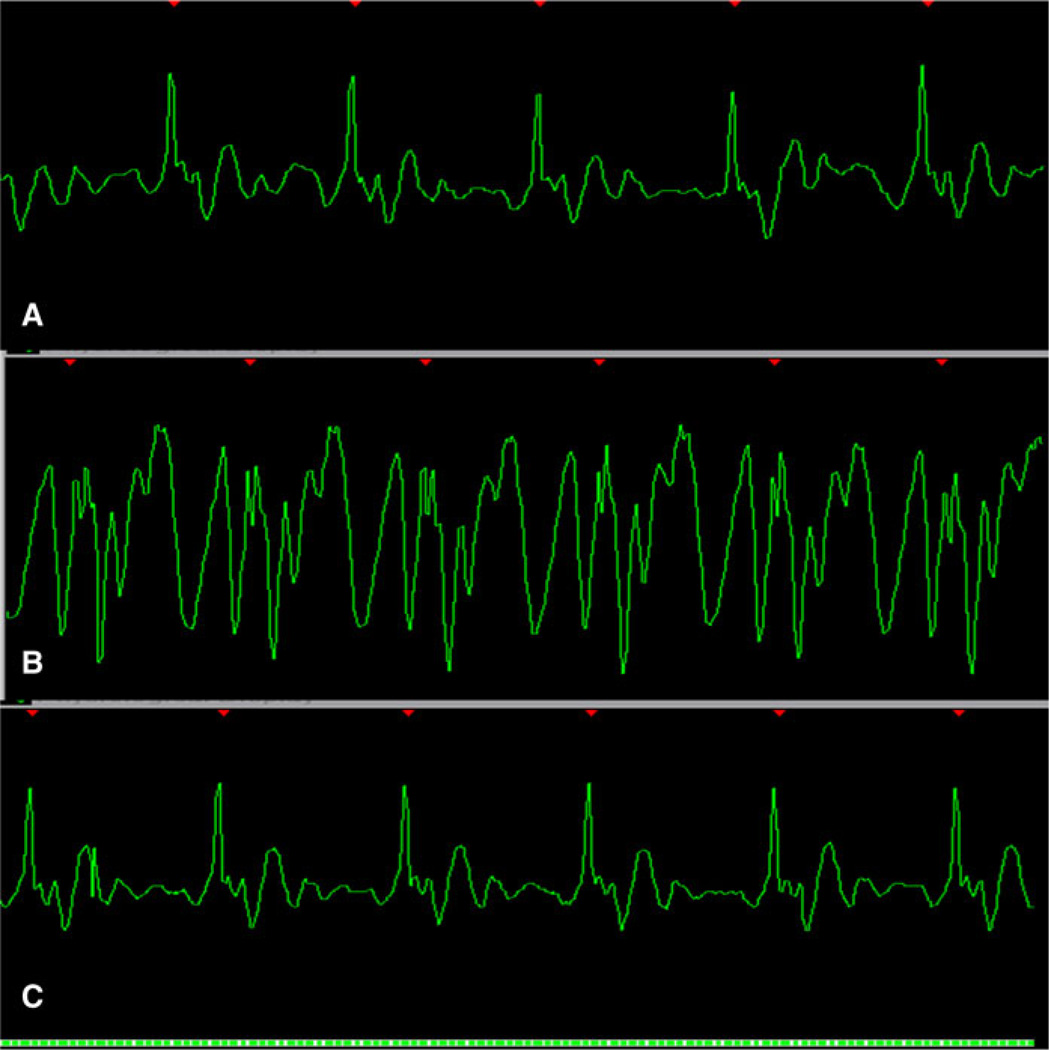
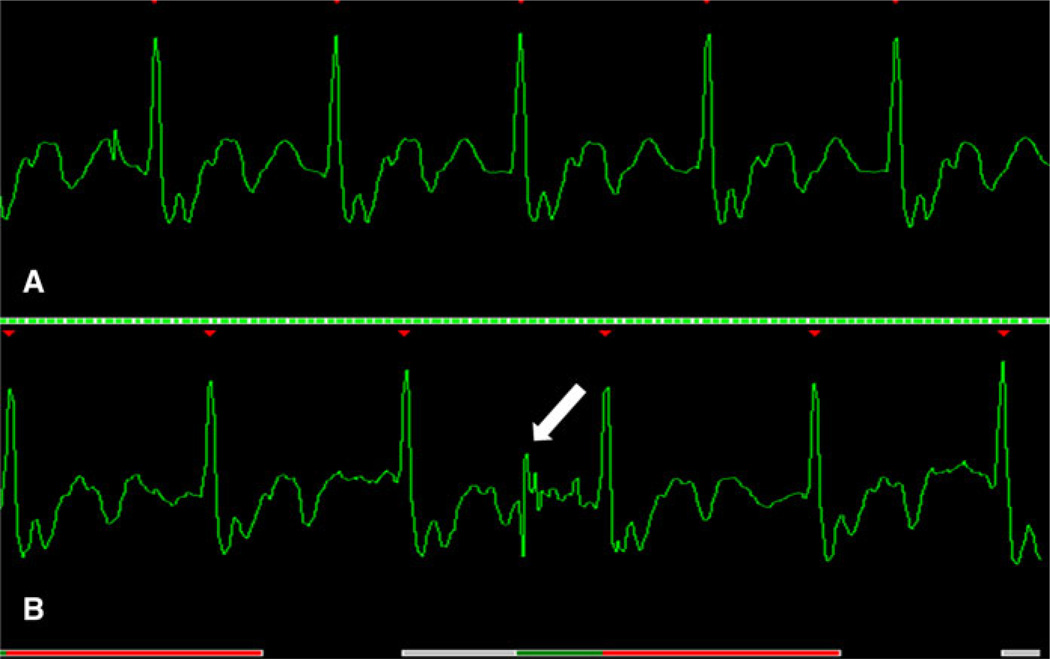
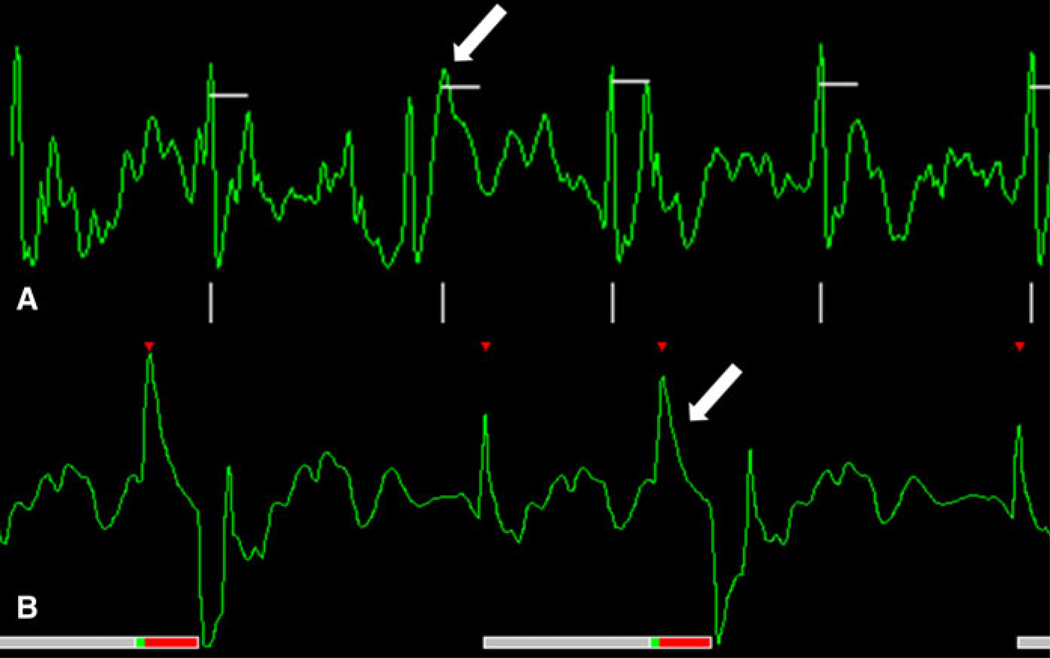
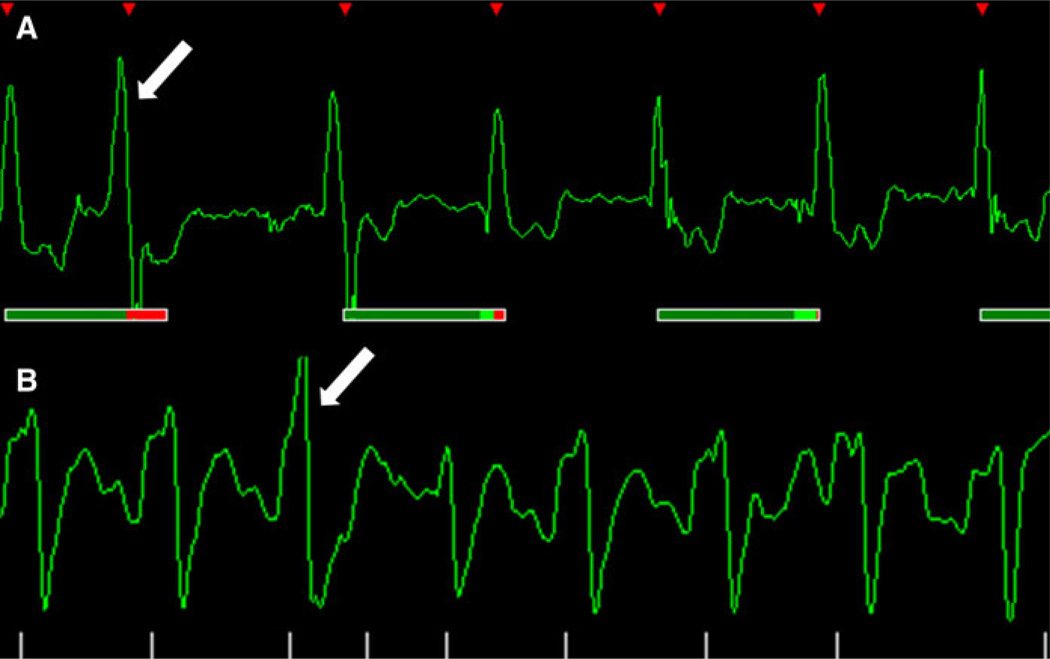
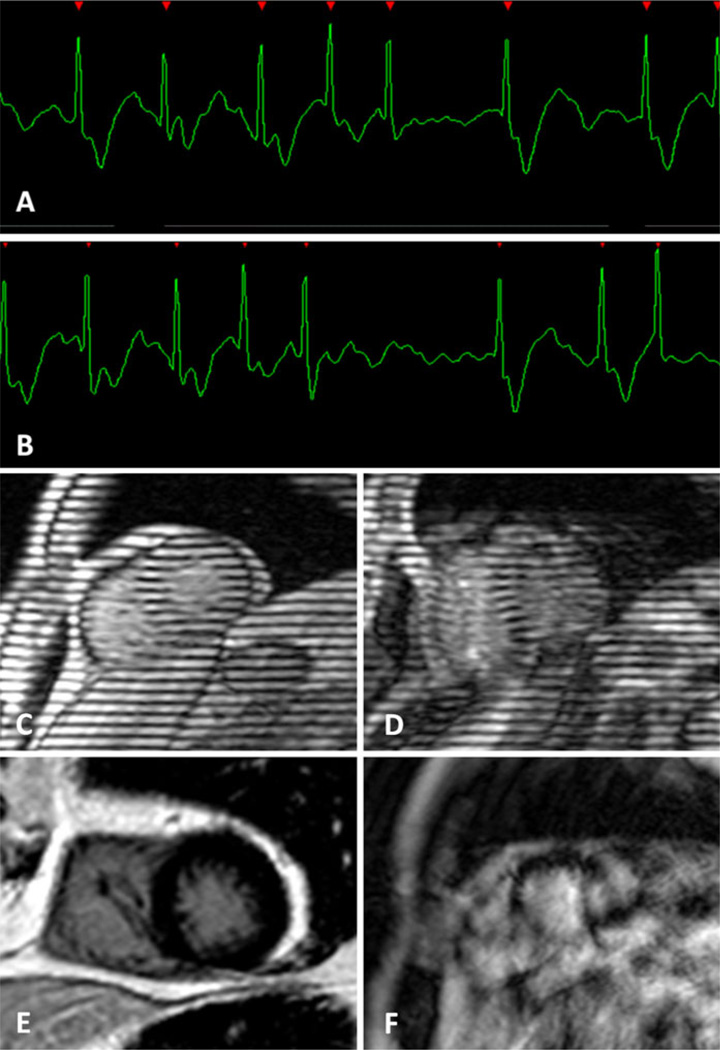
All cardiac magnetic resonance (CMR) techniques aim to create still depictions of a dynamic and ever-adapting organ. Most CMR methods rely on cardiac gating to capture information during fleeting periods of relative cardiac quiescence, at end diastole or end systole, or to acquire partial images throughout the cardiac cycle and average these signals over several heart beats. Since the inception of clinical CMR in the early 1980s, priority has been given to improving methods for image gating. The aim of this work is to provide a basic understanding of the ECG acquisition, demonstrate common ECG-related artifacts and to provide practical methods for overcoming these issues. Meticulous ECG preparation is essential for optimal CMR acquisition and these techniques must be adaptable to the individual patient.
Conflict of interest statement
Figures
References
-
- Lanzer P, Botvinick EH, Schiller NB, et al. Cardiac imaging using gated magnetic resonance. Radiology. 1984;150:121–127. - PubMed
-
- Amoore JN, Ridgway JP. A system for cardiac and respiratory gating of a magnetic resonance imager. Clin Phys Physiol Meas. 1989;10:283–286. - PubMed
-
- McNamara MT, Higgins CB. Cardiovascular applications of magnetic resonance imaging. Magn Reson Imaging. 1984;2:167–183. - PubMed
-
- Osbakken M, Yuschok T. Evaluation of ventricular function with gated cardiac magnetic resonance imaging. Cathet Cardiovasc Diagn. 1986;12:156–160. - PubMed
-
- Stark DD, Higgins CB, Lanzer P, et al. Magnetic resonance imaging of the pericardium: normal and pathologic findings. Radiology. 1984;150:469–474. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
