

Elevated soluble Flt1 inhibits endothelial repair in PR3-ANCA-associated vasculitis
- PMID: 22034638
- PMCID: PMC3269927
- DOI: 10.1681/ASN.2010080858
Elevated soluble Flt1 inhibits endothelial repair in PR3-ANCA-associated vasculitis
Abstract
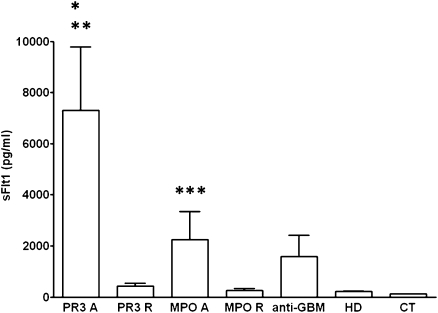
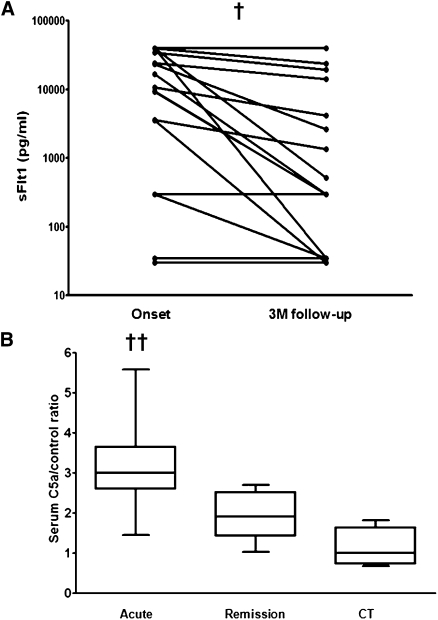
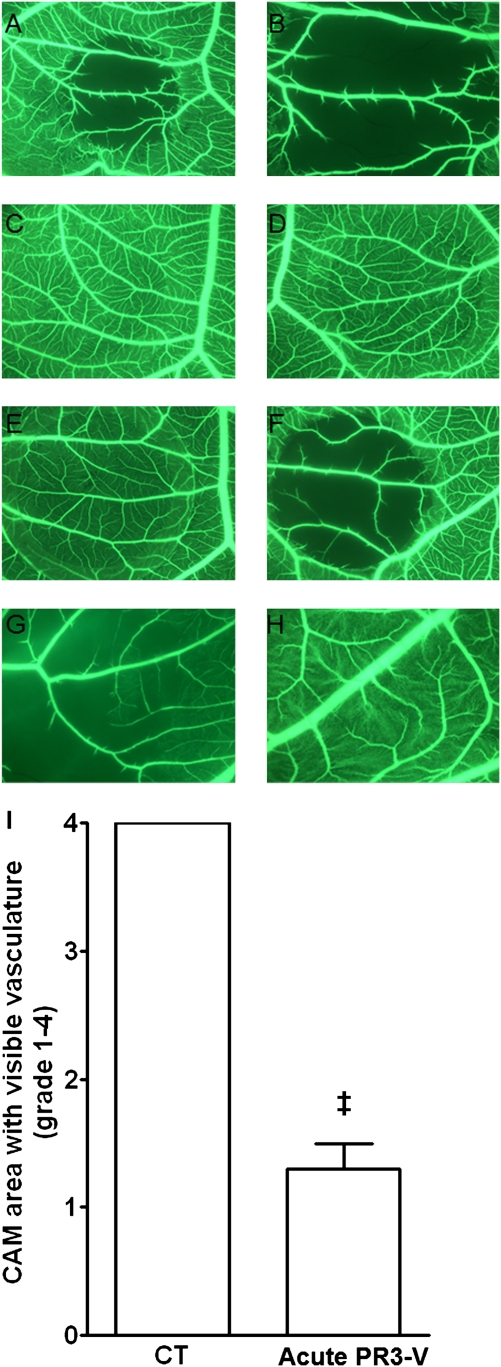
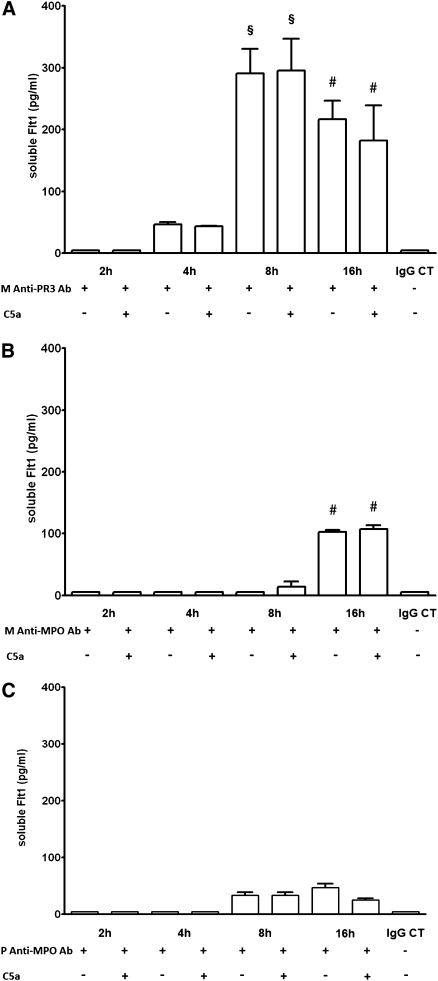
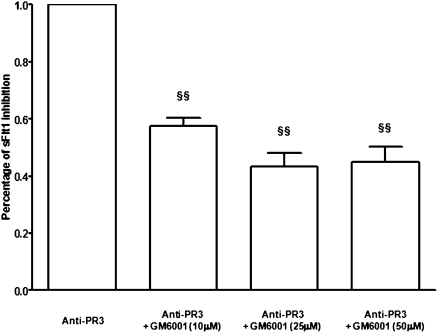
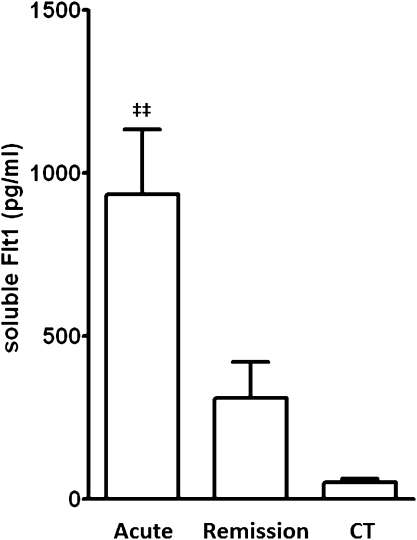
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis exhibits endothelial damage, but the capacity for vessel repair in this disorder is not well understood. Here, we observed a marked increase in serum levels of soluble Flt1 (sFlt1), a potent inhibitor of vascular endothelial growth factor, in patients with active ANCA-associated vasculitis compared with patients during remission and other controls. Serum levels of sFlt1 correlated with C5a, an anaphylatoxin released after complement activation. Serum from patients with acute ANCA-associated vasculitis disrupted blood flow in the chicken chorioallantoic membrane assay, suggesting an antiangiogenic effect. Preincubation with excess human vascular endothelial growth factor prevented this effect. Anti-proteinase-3 (PR3) mAb and serum containing PR3-ANCA from patients with active vasculitis both induced a significant and sustained release of sFlt1 from monocytes, whereas anti-myeloperoxidase (MPO) mAb or polyclonal antibodies did not. However, the serum containing polyclonal PR3-ANCA did not induce release of sFlt1 from cultured human umbilical vein endothelial cells. In summary, these data suggest that anti-PR3 antibodies, and to a much lesser extent anti-MPO antibodies, increase sFlt1 during acute ANCA-associated vasculitis, leading to an antiangiogenic state that hinders endothelial repair.
Figures

Comment in
-
Vasculitis is an antiangiogenic state.J Am Soc Nephrol. 2012 Jan;23(1):8-10. doi: 10.1681/ASN.2011111116. Epub 2011 Dec 15. J Am Soc Nephrol. 2012. PMID: 22173697 No abstract available.
References
-
- Salama AD, Pusey CD: Shining a LAMP on pauci-immune focal segmental glomerulonephritis. Kidney Int 76: 15–17, 2009 - PubMed
-
- van Rossum AP, Rarok AA, Huitema MG, Fassina G, Limburg PC, Kallenberg CG: Constitutive membrane expression of proteinase 3 (PR3) and neutrophil activation by anti-PR3 antibodies. J Leukoc Biol 76: 1162–1170, 2004 - PubMed
-
- Nowack R, Schwalbe K, Flores-Suárez LF, Yard B, van der Woude FJ: Upregulation of CD14 and CD18 on monocytes in vitro by antineutrophil cytoplasmic autoantibodies. J Am Soc Nephrol 11: 1639–1646, 2000 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
