

Esophageal perforation: diagnostic work-up and clinical decision-making in the first 24 hours
- PMID: 22035338
- PMCID: PMC3219576
- DOI: 10.1186/1757-7241-19-66
Esophageal perforation: diagnostic work-up and clinical decision-making in the first 24 hours
Abstract
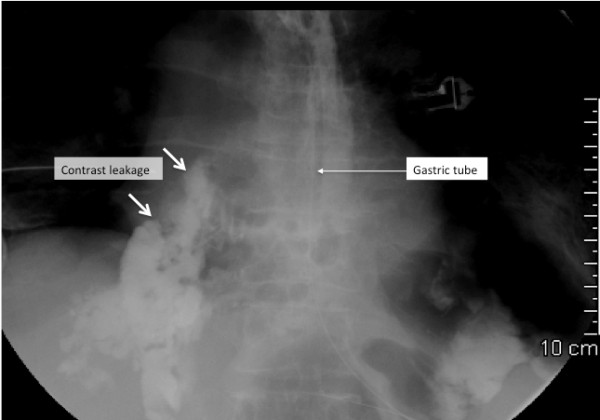
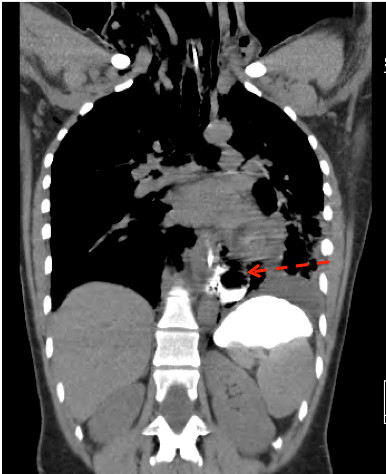
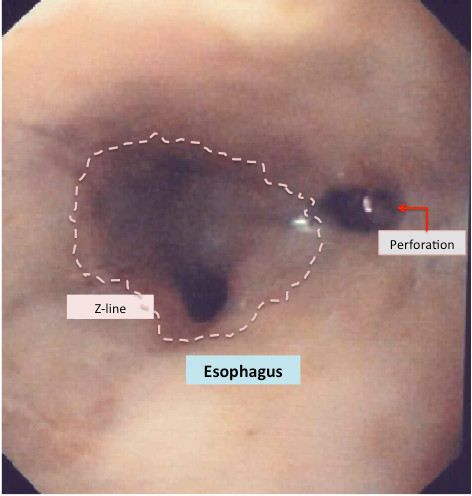
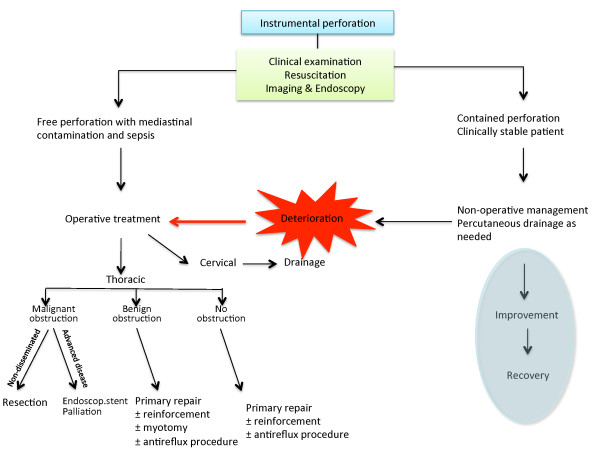
Esophageal perforation is a rare and potentially life-threatening condition. Early clinical suspicion and imaging is important for case management to achieve a good outcome. However, recent studies continue to report high morbidity and mortality greater than 20% from esophageal perforation. At least half of the perforations are iatrogenic, mostly related to endoscopic instrumentation used in the upper gastrointestinal tract, while about a third are spontaneous perforations. Surgical treatment remains an important option for many patients, but a non-operative approach, with or without use of an endoscopic stent or placement of internal or external drains, should be considered when the clinical situation allows for a less invasive approach. The rarity of this emergency makes it difficult for a physician to obtain extensive individual clinical experience; it is also challenging to obtain firm scientific evidence that informs patient management and clinical decision-making. Improved attention to non-specific symptoms and signs and early diagnosis based on imaging may translate into better outcomes for this group of patients, many of whom are elderly with significant comorbidity.
Figures
References
-
- Ryom P, Ravn JB, Penninga L, Schmidt S, Iversen MG, Skov-Olsen P, Kehlet H. Aetiology, treatment and mortality after oesophageal perforation in Denmark. Dan Med Bull. 2011;58:A4267. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
