

Comparison of midwife-led and consultant-led care of healthy women at low risk of childbirth complications in the Republic of Ireland: a randomised trial
- PMID: 22035427
- PMCID: PMC3226589
- DOI: 10.1186/1471-2393-11-85
Comparison of midwife-led and consultant-led care of healthy women at low risk of childbirth complications in the Republic of Ireland: a randomised trial
Abstract
Background: No midwifery-led units existed in Ireland before 2004. The aim of this study was to compare midwife-led (MLU) versus consultant-led (CLU) care for healthy, pregnant women without risk factors for labour and delivery.
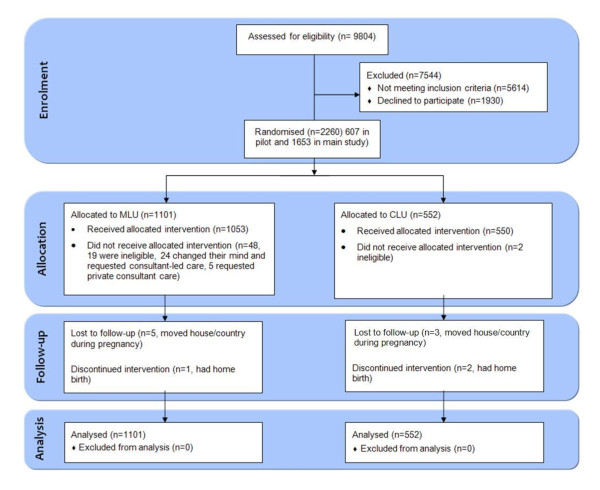
Methods: An unblinded, pragmatic randomised trial was designed, funded by the Health Service Executive (Dublin North-East). Following ethical approval, all women booking prior to 24 weeks of pregnancy at two maternity hospitals with 1,300-3,200 births annually in Ireland were assessed for trial eligibility.1,653 consenting women were centrally randomised on a 2:1 ratio to MLU or CLU care, (1101:552). 'Intention-to-treat' analysis was used to compare 9 key neonatal and maternal outcomes.
Results: No statistically significant difference was found between MLU and CLU in the seven key outcomes: caesarean birth (163 [14.8%] vs 84 [15.2%]; relative risk (RR) 0.97 [95% CI 0.76 to 1.24]), induction (248 [22.5%] vs 138 [25.0%]; RR 0.90 [0.75 to 1.08]), episiotomy (126 [11.4%] vs 68 [12.3%]; RR 0.93 [0.70 to 1.23]), instrumental birth (139 [12.6%] vs 79 [14.3%]; RR 0.88 [0.68 to 1.14]), Apgar scores < 8 (10 [0.9%] vs 9 [1.6%]; RR 0.56 [0.23 to 1.36]), postpartum haemorrhage (144 [13.1%] vs 75 [13.6%]; RR 0.96 [0.74 to 1.25]); breastfeeding initiation (616 [55.9%] vs 317 [57.4%]; RR 0.97 [0.89 to 1.06]). MLU women were significantly less likely to have continuous electronic fetal monitoring (397 [36.1%] vs 313 [56.7%]; RR 0.64 [0.57 to 0.71]), or augmentation of labour (436 [39.6%] vs 314 [56.9%]; RR 0.50 [0.40 to 0.61]).
Conclusions: Midwife-led care, as practised in this study, is as safe as consultant-led care and is associated with less intervention during labour and delivery.
Comment in
-
Midwife-led care is safe in Ireland.Midwives. 2012;15(1):21. Midwives. 2012. PMID: 24868667 No abstract available.
References
-
- Economic and Social Research Institute. Perinatal Statistics Report 2009. Dublin: Economic and Social Research Institute; 2011.
-
- Wagner M. Fish can't see water: the need to humanize birth. Int J Gynaecol Obstet. 2001;75:S25–37. - PubMed
-
- Wagner M. Pursuing the birth machine: the search for appropriate birth technology. Sevenoaks, Kent: ACE Graphics; 1994.
-
- Smyth RMD, Alldred SK, Markham C. Amniotomy for shortening spontaneous labour. Cochrane Database Syst Rev. 2007. p. CD006167. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
