

Costaining for keratins 8/18 plus ubiquitin improves detection of hepatocyte injury in nonalcoholic fatty liver disease
- PMID: 22036053
- PMCID: PMC3288773
- DOI: 10.1016/j.humpath.2011.07.007
Costaining for keratins 8/18 plus ubiquitin improves detection of hepatocyte injury in nonalcoholic fatty liver disease
Abstract
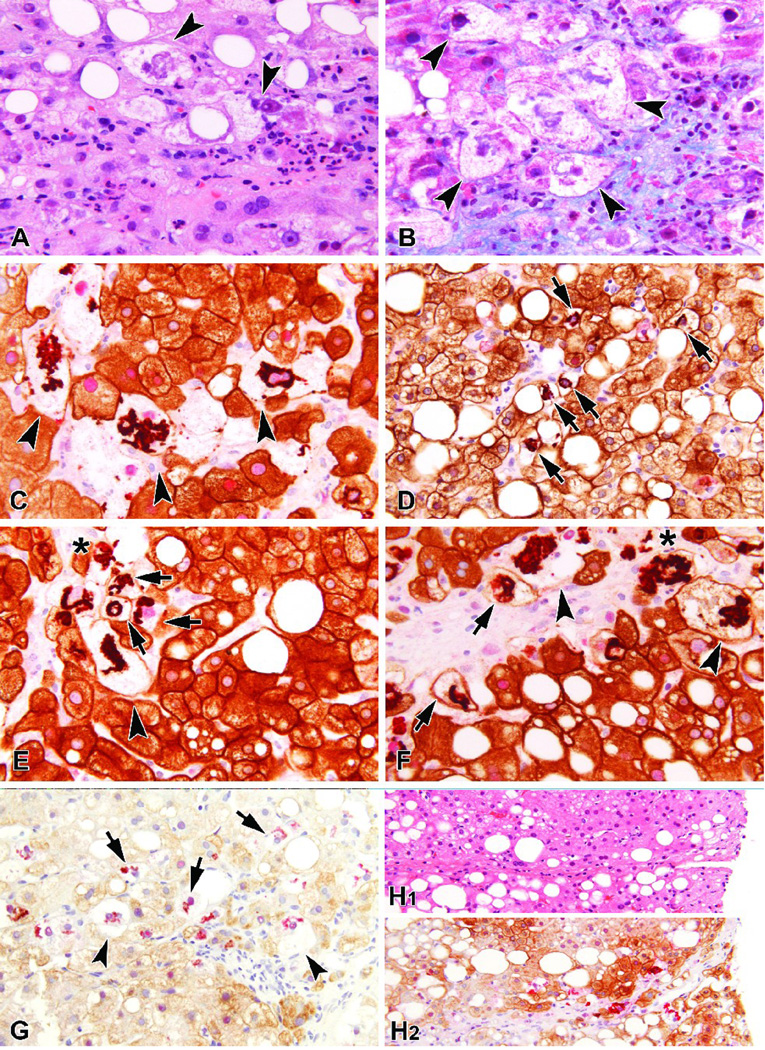
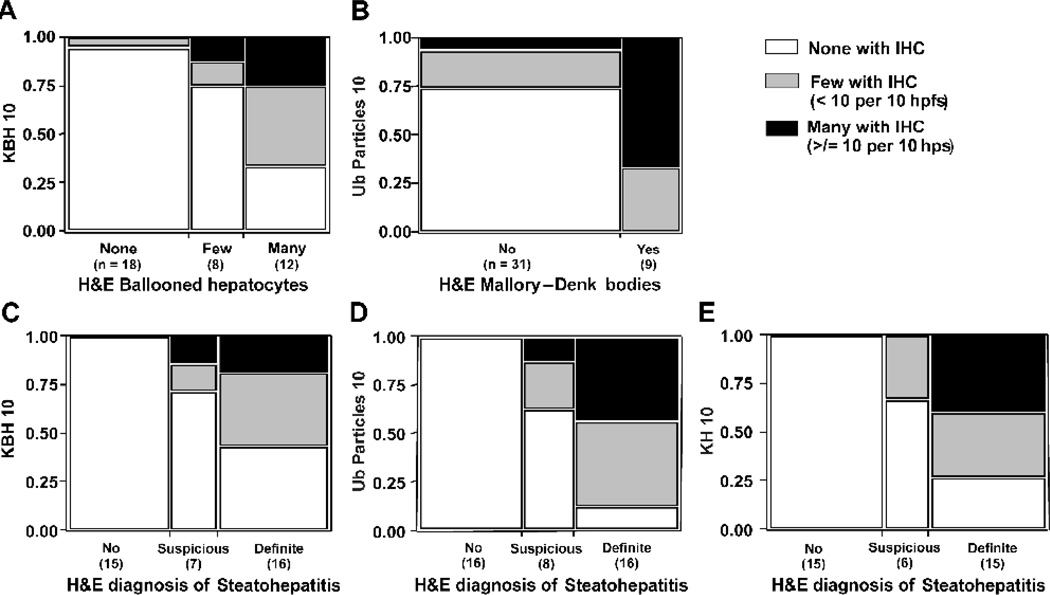
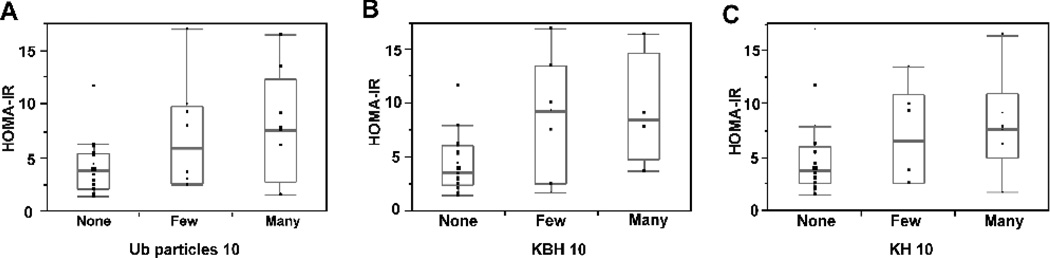
Nonalcoholic fatty liver disease is a global health dilemma. The gold standard for diagnosis is liver biopsy. Ballooned hepatocytes are histologic manifestations of hepatocellular injury and are characteristic of steatohepatitis, the more severe form of nonalcoholic fatty liver disease. Definitive histologic identification of ballooned hepatocytes on routine stains, however, can be difficult. Immunohistochemical evidence for loss of the normal hepatocytic keratin 8/18 can serve as an objective marker of ballooned hepatocytes. We sought to explore the utility of a keratin 8/18 plus ubiquitin double immunohistochemical stain for the histologic evaluation of adult nonalcoholic fatty liver disease. Double immunohistochemical staining for keratin 8/18 and ubiquitin was analyzed using 40 adult human nonalcoholic fatty liver disease core liver biopsies. Ballooned hepatocytes lack keratin 8/18 staining as previously shown by others, but normal-size hepatocytes with keratin loss are approximately 5 times greater in number than keratin-negative ballooned hepatocytes. Keratin-negative ballooned hepatocytes, normal-size hepatocytes with keratin loss, and ubiquitin deposits show a zonal distribution, are positively associated with each other, and are frequently found adjacent to or intermixed with fibrous matrix. All 3 lesions correlate with fibrosis stage and the hematoxylin and eosin diagnosis of steatohepatitis (all P < .05). Compared with hematoxylin and eosin staining, immunohistochemical staining improves the receiver operating characteristics curve for advanced fibrosis (0.77 versus 0.83, 0.89, and 0.89 for keratin-negative ballooned hepatocytes, normal-size hepatocytes with keratin loss, and ubiquitin, respectively) because immunohistochemistry is more sensitive and specific for fibrogenic hepatocellular injury than hematoxylin and eosin staining. Keratin 8/18 plus ubiquitin double immunohistochemical stain improves detection of hepatocyte injury in nonalcoholic fatty liver disease. Thus, it may help differentiate nonalcoholic steatohepatitis from nonalcoholic fatty liver.
Copyright © 2012 Elsevier Inc. All rights reserved.
Figures
References
-
- Matteoni CA, Younossi ZM, Gramlich T, Boparai N, Liu YC, McCullough AJ. Nonalcoholic fatty liver disease: a spectrum of clinical and pathological severity. Gastroenterology. 1999;116:1413–1419. - PubMed
-
- Sanyal AJ. AGA technical review on nonalcoholic fatty liver disease. Gastroenterology. 2002;123:1705–1725. - PubMed
-
- McCullough AJ. Update on nonalcoholic fatty liver disease. J Clin Gastroenterol. 2002;34:255–262. - PubMed
-
- Adams LA, Lindor KD. Nonalcoholic fatty liver disease. Ann Epidemiol. 2007;17:863–869. - PubMed
-
- Starley BQ, Calcagno CJ, Harrison SA. Nonalcoholic fatty liver disease and hepatocellular carcinoma: a weighty connection. Hepatology. 2010;51:1820–1832. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UL1RR02501401/RR/NCRR NIH HHS/United States
- U01DK061713/DK/NIDDK NIH HHS/United States
- U01 DK061732/DK/NIDDK NIH HHS/United States
- U01DK061731/DK/NIDDK NIH HHS/United States
- U01DK061737/DK/NIDDK NIH HHS/United States
- M01 RR000188/RR/NCRR NIH HHS/United States
- U01DK061718/DK/NIDDK NIH HHS/United States
- U01DK061728/DK/NIDDK NIH HHS/United States
- U01 DK061730/DK/NIDDK NIH HHS/United States
- U01 DK061728/DK/NIDDK NIH HHS/United States
- U01 DK061734/DK/NIDDK NIH HHS/United States
- M01RR020359/RR/NCRR NIH HHS/United States
- M01RR000827/RR/NCRR NIH HHS/United States
- U01DK061738/DK/NIDDK NIH HHS/United States
- U01 DK061737/DK/NIDDK NIH HHS/United States
- U01 DK061713/DK/NIDDK NIH HHS/United States
- UL1 RR024989/RR/NCRR NIH HHS/United States
- U01 DK061731/DK/NIDDK NIH HHS/United States
- UL1RR02413101/RR/NCRR NIH HHS/United States
- U01 DK061718/DK/NIDDK NIH HHS/United States
- M01RR000065/RR/NCRR NIH HHS/United States
- U01DK061732/DK/NIDDK NIH HHS/United States
- M01 RR000750/RR/NCRR NIH HHS/United States
- K23-DK062116/DK/NIDDK NIH HHS/United States
- M01 RR000065/RR/NCRR NIH HHS/United States
- K23 DK062116/DK/NIDDK NIH HHS/United States
- UL1RR024989/RR/NCRR NIH HHS/United States
- U01 DK061738/DK/NIDDK NIH HHS/United States
- R01 DK077794/DK/NIDDK NIH HHS/United States
- M01 RR000827/RR/NCRR NIH HHS/United States
- M01RR00188/RR/NCRR NIH HHS/United States
- U01DK061734/DK/NIDDK NIH HHS/United States
- U01DK061730/DK/NIDDK NIH HHS/United States
- M01 RR020359/RR/NCRR NIH HHS/United States
- M01RR000750/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
