

Immediate changes in intraocular pressure after laser peripheral iridotomy in primary angle-closure suspects
- PMID: 22036632
- PMCID: PMC3570569
- DOI: 10.1016/j.ophtha.2011.08.014
Immediate changes in intraocular pressure after laser peripheral iridotomy in primary angle-closure suspects
Abstract
Purpose: To determine the immediate changes in intraocular pressure (IOP) after laser peripheral iridotomy in primary angle-closure suspects.
Design: Prospective, randomized controlled trial (split-body design).
Participants: Seven hundred thirty-four Chinese people 50 to 70 years of age.
Methods: Primary angle-closure suspects underwent iridotomy using a neodymium:yttrium-aluminum-garnet laser in 1 randomly selected eye, with the fellow eye serving as a control. Intraocular pressure was measured using Goldmann applanation tonometry before treatment and 1 hour and 2 weeks after treatment. Total energy used and complications were recorded. Risk factors for IOP rise after laser peripheral iridotomy were investigated.
Main outcome measures: Intraocular pressure.
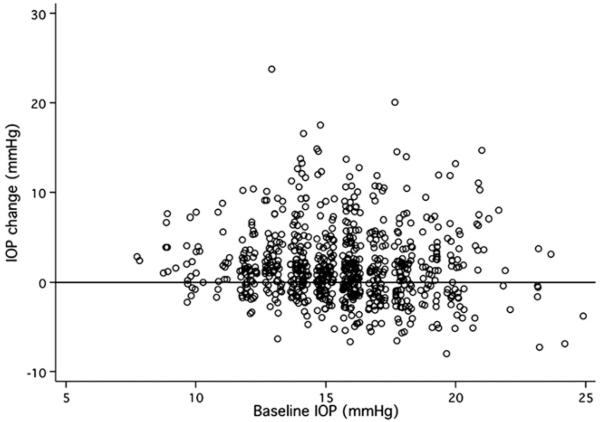
Results: The proportion of treated eyes with an IOP spike (an elevation of ≥8 mmHg more than baseline) at 1 hour and 2 weeks after treatment was 9.8% (95% confidence interval [CI], 7.7-12.0) and 0.82% (95% CI, 0.2-1.5), respectively. Only 4 (0.54%) of 734 eyes (95% CI, 0.01-1.08) had an immediate posttreatment IOP of 30 mmHg or more and needed medical intervention. The average IOP 1 hour after treatment was 17.5±4.7 mmHg in the treated eyes, as compared with 15.2±2.6 mmHg in controls. At 2 weeks after treatment, these values were 15.6±3.4 mmHg in treated eyes and 15.1±2.7 mmHg in controls (P<0.001). No significant difference was detected in the baseline IOP of the treated and untreated eyes. Logistic regression showed that the incidence of IOP spike was associated with greater laser energy used and shallower central anterior chamber.
Conclusions: Laser peripheral iridotomy in primary angle-closure suspects resulted in significant IOP rise in 9.8% and 0.82% of cases at 1 hour and 2 weeks, respectively. Eyes in which more laser energy and a higher number of laser pulses were used and those with shallower central anterior chambers were at increased risk for IOP spikes at 1 hour after laser peripheral iridotomy.
Copyright © 2012 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Laser peripheral iridotomy for pupillary-block glaucoma. Ophthalmology. 1989;96(suppl):218–28. - PubMed
-
- American Academy of Ophthalmology Laser peripheral iridotomy for pupillary-block glaucoma. Ophthalmology. 1994;101:1749–58. - PubMed
-
- Aung T, Ang LP, Chan SP, Chew PT. Acute primary angle-closure: long-term intraocular pressure outcome in Asian eyes. Am J Ophthalmol. 2001;131:7–12. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
