

Validation of a common data model for active safety surveillance research
- PMID: 22037893
- PMCID: PMC3240764
- DOI: 10.1136/amiajnl-2011-000376
Validation of a common data model for active safety surveillance research
Abstract
Objective: Systematic analysis of observational medical databases for active safety surveillance is hindered by the variation in data models and coding systems. Data analysts often find robust clinical data models difficult to understand and ill suited to support their analytic approaches. Further, some models do not facilitate the computations required for systematic analysis across many interventions and outcomes for large datasets. Translating the data from these idiosyncratic data models to a common data model (CDM) could facilitate both the analysts' understanding and the suitability for large-scale systematic analysis. In addition to facilitating analysis, a suitable CDM has to faithfully represent the source observational database. Before beginning to use the Observational Medical Outcomes Partnership (OMOP) CDM and a related dictionary of standardized terminologies for a study of large-scale systematic active safety surveillance, the authors validated the model's suitability for this use by example.
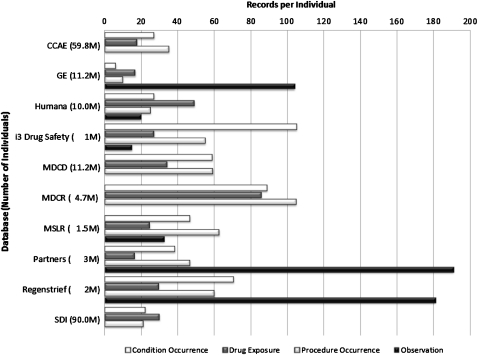
Validation by example: To validate the OMOP CDM, the model was instantiated into a relational database, data from 10 different observational healthcare databases were loaded into separate instances, a comprehensive array of analytic methods that operate on the data model was created, and these methods were executed against the databases to measure performance.
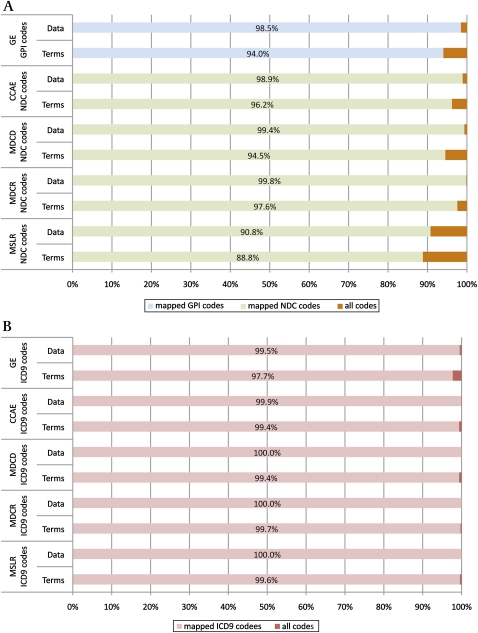
Conclusion: There was acceptable representation of the data from 10 observational databases in the OMOP CDM using the standardized terminologies selected, and a range of analytic methods was developed and executed with sufficient performance to be useful for active safety surveillance.
Conflict of interest statement
Figures
References
-
- Benson K, Hartz AJ. A comparison of observational studies and randomized, controlled trials. N Engl J Med 2000;342:1878–86 - PubMed
-
- Moses LE. Measuring effects without randomized trials? Options, problems, challenges. Med Care 1995;33(4 suppl):AS8–14 - PubMed
-
- Stang PE, Ryan PB, Racoosin JA, et al. Advancing the science for active surveillance: rationale and design for the observational medical outcomes partnership. Ann Intern Med 2010;153:600–6 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
