

doi: 10.1007/s00261-011-9818-6.
High-risk prostate cancer: value of multi-modality 3T MRI-guided biopsies after previous negative biopsies
Affiliations
- PMID: 22038330
- PMCID: PMC3449056
- DOI: 10.1007/s00261-011-9818-6
Item in Clipboard
High-risk prostate cancer: value of multi-modality 3T MRI-guided biopsies after previous negative biopsies
Abdom Imaging.
2012 Oct.
Abstract
Transrectal ultrasound-guided biopsy is the gold standard for prostate cancer detection. The latter detection rates of random systematic TRUS-guided biopsy do not exceed 44%. As a consequence other biopsy methods have been explored. One of these methods is MR-guided biopsy (MRGB), which revealed detection rates of 38-59% after previous negative TRUSGB sessions. For this reason MRGB will probably become more and more applied in daily practice.
Figures
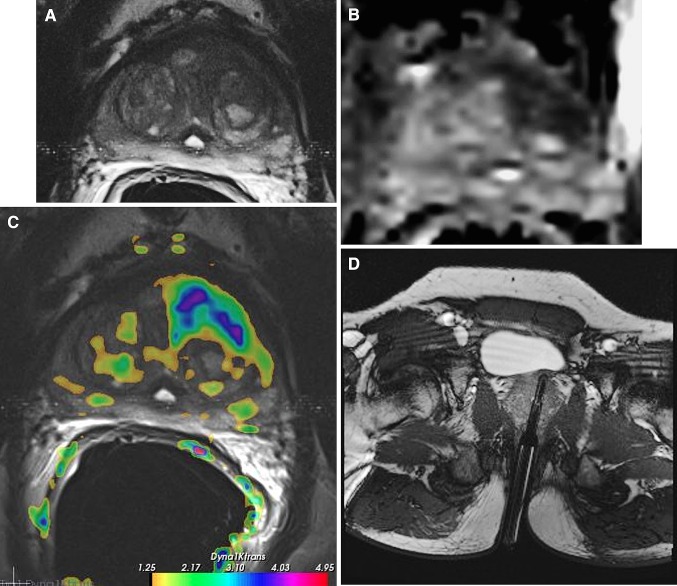
Multi-parametric MR images, comprising T2-weighted (A), diffusion weighted-derived apparent diffusion coefficient map image (B), and dynamic contrast-enhanced image (Ktrans) (C), in a 63 year old male, with a PSA of 12 ng/ml, and a history of two negative transrectal ultrasound guided prostate biopsy sessions. In the left transitional zone a cancer suspicious region is present (low-signal intensity lesion on T2, asymmetric Ktrans and restricted diffusion on the ADC map). D During a second session, a MR-guided biopsy was performed of the cancer suspicious area. The needle guider was pointed toward the cancer suspicious region in axial and subsequently biopsied. Verification image with the needle guider left in situ was obtained. Histopathology revealed a Gleason 4 + 3 prostate cancer.
References
-
- Hricak H. MR imaging and MR spectroscopic imaging in the pre-treatment evaluation of prostate cancer. Br J Radiol. 2005;78(2):S103–S111. - PubMed
-
- Thompson IM, Seay TM. Will current clinical trials answer the most important questions about prostate adenocarcinoma? Oncology (Williston Park) 1997;11:1109–1117. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
