

Magnetic resonance evaluation of tubercular lesion in spine
- PMID: 22038440
- PMCID: PMC3282842
- DOI: 10.1007/s00264-011-1380-x
Magnetic resonance evaluation of tubercular lesion in spine
Abstract
Purpose: Information on Magnetic Resonance (MR) features of active and healed lesions in tuberculosis (TB) spine are lacking. We evaluated MRI findings in active and healed proven TB spine to establish the diagnostic features.
Materials and method: Forty-nine consecutive spinal TB patients (20 male; 29 female) diagnosed clinicoradiologically and/or on histopathology, Fine Needle Aspiration Cytology (FNAC), bacteriology, or Polymerase Chain Reaction (PCR) were enrolled. Pretreatment MR scans were reviewed for diagnostic features, and eight-month follow-up MR scans were reviewed for healing changes.
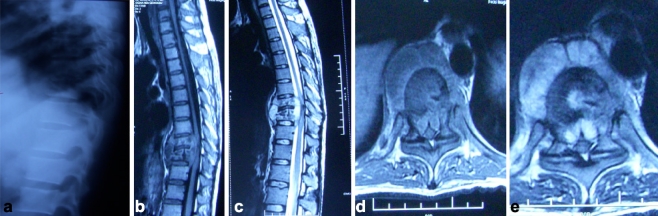
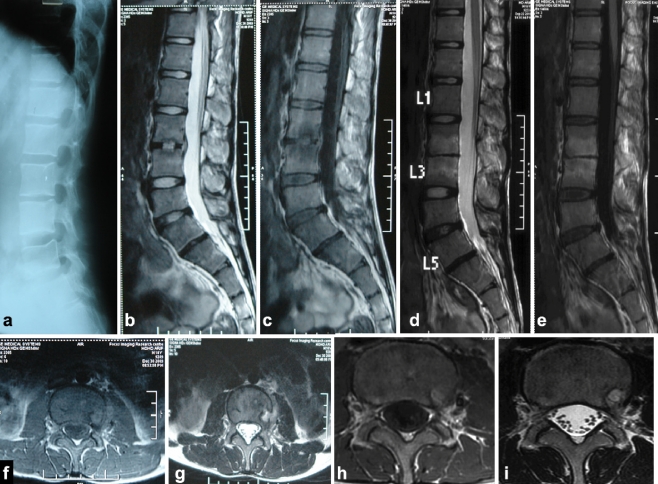
Results: Cervical spine (n = 6), dorsal spine (n = 14), and lumbar spine (n = 29) were affected. Fourteen had paraplegia. Mean vertebrae involved were 2.61 on X-ray with a total of 128 vertebrae (VB) and 3.2 on MRI (range, 2-15) with 161 VB. The lesions were more extensive on MRI (34.7%) than appreciated on X-ray. The disc was preserved partially or fully in 88.2% of instances. End plate erosions (159/161 VB), lost VB height (94/161), exudative lesion (158/161), granular lesion (3/161), pre and paravertebral collections (49/49 cases), marrow oedema (161/161), discitis (98%), epidural involvement (107/161), epidural spread (100/161), and subligamentous spread (156/161) were observed. Canal encroachment (10-90%) was seen in 37 cases. Mean motor and sensory scores with greater than 50% canal encroachment were 87/100 and 156/168, respectively. Cord oedema was observed in 11 cases (eight with neural deficit and three cases without). Cord atrophy was seen in one case each before and after treatment. A total of 83% of patients had a combination of paravertebral collections, marrow oedema, subligamentous and epidural extension, endplate erosions and discitis. On healing (n = 20), complete resolution of marrow oedema and collections, fatty replacement of bone marrow and resolution of cord signal intensity were observed.
Conclusion: The marrow oedema, preservation of disc space, subligamentous extension of abscess, septate paravertebral abscess, epidural extension, endplate erosions and discitis were consistently observed in 83% cases of TB spine on MRI.
Figures

References
-
- Desai SS. Early diagnosis of spinal tuberculosis by MRI. J Bone Joint Surg Br. 1994;76(6):863–869. - PubMed
-
- Sharif HS, Clark DC, Aabed MY, Haddad MC, al Deeb SM, Yaqub B, al Moutaery KR. Granulomatous spinal infections: MR imaging. Radiology. 1990;177(1):101–107. - PubMed
-
- Jain AK (2002) Treatment of tuberculosis of the spine with neurologic complications. Clin Orthop Relat Res (398):75–84 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
