

Mutations of the SF3B1 splicing factor in chronic lymphocytic leukemia: association with progression and fludarabine-refractoriness
- PMID: 22039264
- PMCID: PMC3245210
- DOI: 10.1182/blood-2011-08-373159
Mutations of the SF3B1 splicing factor in chronic lymphocytic leukemia: association with progression and fludarabine-refractoriness
Abstract
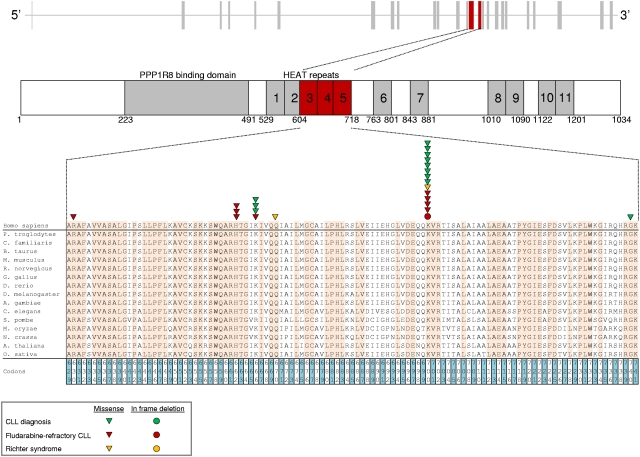
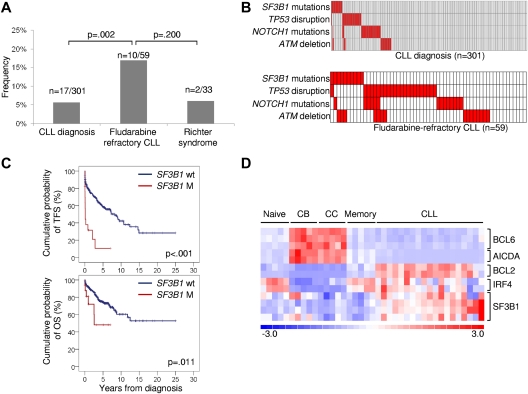
The genetic lesions identified in chronic lymphocytic leukemia (CLL) do not entirely recapitulate the disease pathogenesis and the development of serious complications, such as chemorefractoriness. While investigating the coding genome of fludarabine-refractory CLL, we observed that mutations of SF3B1, encoding a splicing factor and representing a critical component of the cell spliceosome, were recurrent in 10 of 59 (17%) fludarabine-refractory cases, with a frequency significantly greater than that observed in a consecutive CLL cohort sampled at diagnosis (17/301, 5%; P = .002). Mutations were somatically acquired, were generally represented by missense nucleotide changes, clustered in selected HEAT repeats of the SF3B1 protein, recurrently targeted 3 hotspots (codons 662, 666, and 700), and were predictive of a poor prognosis. In fludarabine-refractory CLL, SF3B1 mutations and TP53 disruption distributed in a mutually exclusive fashion (P = .046). The identification of SF3B1 mutations points to splicing regulation as a novel pathogenetic mechanism of potential clinical relevance in CLL.
Figures
References
-
- Müller-Hermelink HK, Montserrat E, Catovsky D, Campo E, Harris NL, Stein H. Chronic lymphocytic leukemia/small lymphocytic lymphoma. In: Swerdlow SH, Campo E, Harris NL, et al., editors. World Health Organization Classification of Tumours, Pathology and Genetics of Tumours of Haematopoietic and Lymphoid Tissues. Lyon, France: IARC; 2008. pp. 180–182.
-
- Hallek M, Cheson BD, Catovsky D, et al. Guidelines for the diagnosis and treatment of chronic lymphocytic leukemia: a report from the International Workshop on Chronic Lymphocytic Leukemia updating the National Cancer Institute—Working Group 1996 guidelines. Blood. 2008;111(12):5446–5456. - PMC - PubMed
-
- Rossi D, Spina V, Deambrogi C, et al. The genetics of Richter syndrome reveals disease heterogeneity and predicts survival after transformation. Blood. 2011;117(12):3391–3401. - PubMed
-
- Chiorazzi N, Rai KR, Ferrarini M. Chronic lymphocytic leukemia. N Engl J Med. 2005;352(8):804–815. - PubMed
-
- Kay NE, O'Brien SM, Pettitt AR, Stilgenbauer S. The role of prognostic factors in assessing ‘high-risk’ subgroups of patients with chronic lymphocytic leukemia. Leukemia. 2007;21(9):1885–1891. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
