

Right ventricular dysfunction is a predictor of non-response and clinical outcome following cardiac resynchronization therapy
- PMID: 22040270
- PMCID: PMC3217913
- DOI: 10.1186/1532-429X-13-68
Right ventricular dysfunction is a predictor of non-response and clinical outcome following cardiac resynchronization therapy
Abstract
Background: Cardiac resynchronization therapy (CRT) is an established treatment in advanced heart failure (HF). However, an important subset does not derive a significant benefit. Despite an established predictive role in HF, the significance of right ventricular (RV) dysfunction in predicting clinical benefit from CRT remains unclear. We investigated the role of RV function, assessed by cardiovascular magnetic resonance (CMR), in predicting response to and major adverse clinical events in HF patients undergoing CRT.
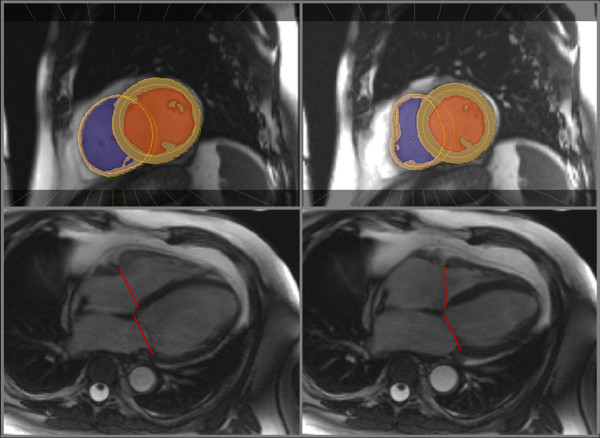
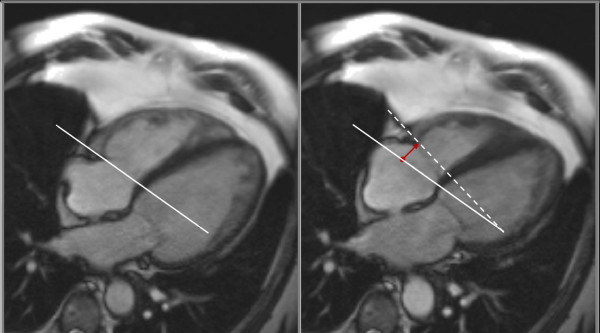
Methods: Sixty consecutive patients were evaluated with CMR prior to CRT implantation in a tertiary cardiac centre. The primary end-point was a composite of death from any cause or unplanned hospitalization for a major cardiovascular event. The secondary end-point was response to therapy, defined as improvement in left ventricular ejection fraction ≥ 5% on echocardiography at one year.
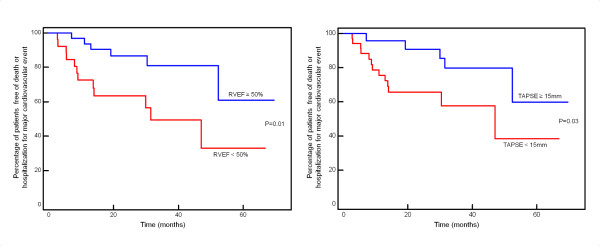
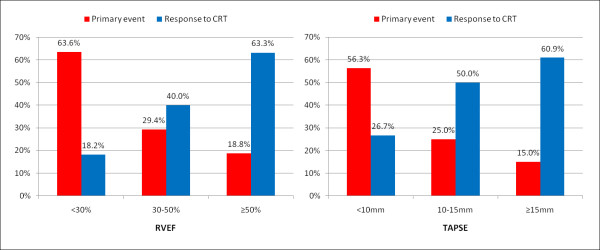
Results: Eighteen patients (30%) met the primary end-point over a median follow-up period of 26 months, and 27 out of 56 patients (48%) were considered responders to CRT. On time-to-event analysis, only atrial fibrillation (HR 2.6, 95% CI 1.02-6.84, p = 0.047) and RV dysfunction, either by a reduced right ventricular ejection fraction-RVEF (HR 0.96, 95% CI 0.94-0.99, p = 0.006) or tricuspid annular plane systolic excursion-TAPSE (HR 0.88, 95% CI, 0.80-0.96, p = 0.006), were significant predictors of adverse events. On logistic regression analysis, preserved RVEF (OR 1.05, 95% CI 1.01-1.09, p = 0.01) and myocardial scar burden (OR 0.90, 95% CI 0.83-0.96, p = 0.004) were the sole independent predictors of response to CRT. Patients with marked RV dysfunction (RVEF < 30%) had a particularly low response rate (18.2%) to CRT.
Conclusions: Right ventricular function is an important predictor of both response to CRT and long-term clinical outcome. Routine assessment of the right ventricle should be considered in the evaluation of patients for CRT.
Figures
References
-
- Cazeau S, Leclercq C, Lavergne T, Walker S, Varma C, Linde C, Garrigue S, Kappenberger L, Haywood GA, Santini M, Bailleul C, Daubert JC. Effects of multisite biventricular pacing in patients with heart failure and intraventricular conduction delay. N Engl J Med. 2001;344:873–80. doi: 10.1056/NEJM200103223441202. - DOI - PubMed
-
- Cleland JG, Daubert JC, Erdmann E, Freemantle N, Gras D, Kappenberger L, Tavazzi L. Cardiac Resynchronization-Heart Failure (CARE-HF) Study Investigators. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med. 2005;352:1539–1549. doi: 10.1056/NEJMoa050496. - DOI - PubMed
-
- Scuteri L, Rordorf R, Marsan NA, Landolina M, Magrini G, Klersy C, Frattini F, Petracci B, Vicentini A, Campana C, Tavazzi L, Ghio S. Relevance of echocardiographic evaluation of right ventricular function in patients undergoing cardiac resynchronization therapy. Pacing Clin Electrophysiol. 2009;32:1040–1049. doi: 10.1111/j.1540-8159.2009.02436.x. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
