

Definitions, criteria and global classification of mast cell disorders with special reference to mast cell activation syndromes: a consensus proposal
- PMID: 22041891
- PMCID: PMC3224511
- DOI: 10.1159/000328760
Definitions, criteria and global classification of mast cell disorders with special reference to mast cell activation syndromes: a consensus proposal
Abstract
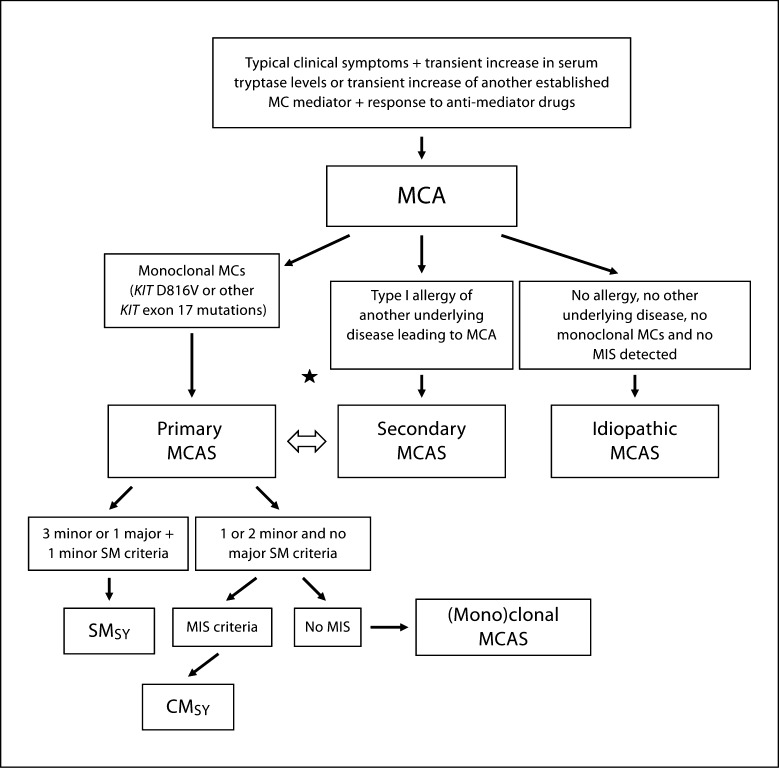
Activation of tissue mast cells (MCs) and their abnormal growth and accumulation in various organs are typically found in primary MC disorders also referred to as mastocytosis. However, increasing numbers of patients are now being informed that their clinical findings are due to MC activation (MCA) that is neither associated with mastocytosis nor with a defined allergic or inflammatory reaction. In other patients with MCA, MCs appear to be clonal cells, but criteria for diagnosing mastocytosis are not met. A working conference was organized in 2010 with the aim to define criteria for diagnosing MCA and related disorders, and to propose a global unifying classification of all MC disorders and pathologic MC reactions. This classification includes three types of 'MCA syndromes' (MCASs), namely primary MCAS, secondary MCAS and idiopathic MCAS. MCA is now defined by robust and generally applicable criteria, including (1) typical clinical symptoms, (2) a substantial transient increase in serum total tryptase level or an increase in other MC-derived mediators, such as histamine or prostaglandin D(2), or their urinary metabolites, and (3) a response of clinical symptoms to agents that attenuate the production or activities of MC mediators. These criteria should assist in the identification and diagnosis of patients with MCAS, and in avoiding misdiagnoses or overinterpretation of clinical symptoms in daily practice. Moreover, the MCAS concept should stimulate research in order to identify and exploit new molecular mechanisms and therapeutic targets.
Copyright © 2011 S. Karger AG, Basel.
Figures
References
-
- Rivera J, Gilfillan AM. Molecular regulation of mast cell activation. J Allergy Clin Immunol. 2006;117:1214–1225. - PubMed
-
- Austen KF. Systemic anaphylaxis in the human being. N Engl J Med. 1974;291:661–664. - PubMed
-
- Serafin WE, Austen KF. Mediators of immediate hypersensitivity reactions. N Engl J Med. 1987;317:30–34. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
