

HIV-infected individuals with co-occurring bipolar disorder evidence poor antiretroviral and psychiatric medication adherence
- PMID: 22041931
- PMCID: PMC3351543
- DOI: 10.1007/s10461-011-0072-2
HIV-infected individuals with co-occurring bipolar disorder evidence poor antiretroviral and psychiatric medication adherence
Abstract
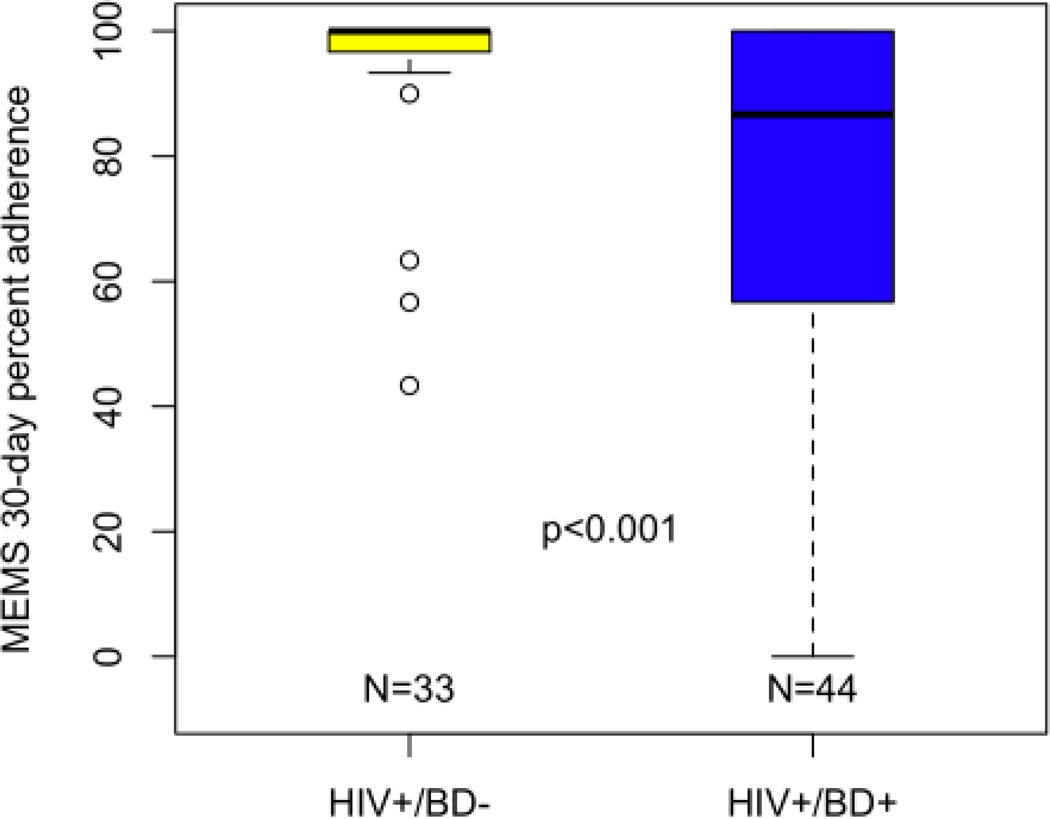
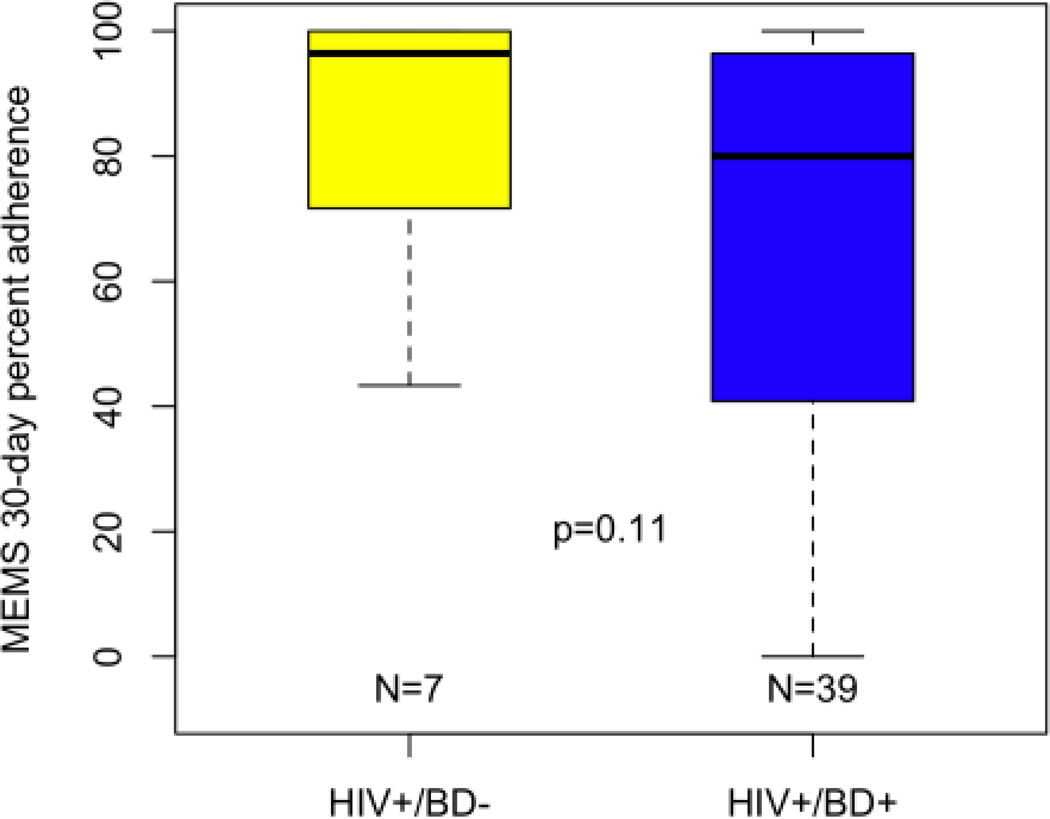
The contribution of bipolar disorder (BD), a prevalent serious mental illness characterized by impulsivity and mood instability, to antiretroviral (ART) and psychiatric medication adherence among HIV-infected (HIV+) individuals is unknown. We examined medication adherence among 44 HIV+/BD+ persons as compared to 33 demographically- and medically-comparable HIV+/BD- persons. Classification of adherent (≥ 90%) or non-adherent (<90%) based on proportion of correctly taken doses over 30 days was determined using electronic medication monitoring devices. HIV+/BD+ persons were significantly less likely to be ART adherent (47.7%) as compared to HIV+/BD- (90.9%) persons. Within the HIV+/BD+ group, mean psychiatric medication adherence was significantly worse than ART medication adherence, although there was a significant correlation between ART and psychiatric adherence levels. Importantly, 30-day ART adherence was associated with plasma virologic response among HIV+/BD+ individuals. Given the high overlap of HIV and BD, and the observed medication adherence difficulties for these persons, specialized adherence improvement interventions are needed.
Figures
References
-
- Gifford AL, Bormann JE, Shively MJ, Wright BC, Richman DD, Bozzette SA. Predictors of self-reported adherence and plasma HIV concentrations in patients on multidrug antiretroviral regimens. J Acquir Immune Defic Syndr. 2000 Apr 15;23(5):386–395. - PubMed
-
- Descamps D, Flandre P, Calvez V, et al. Mechanisms of virologic failure in previously untreated HIV-infected patients from a trial of induction-maintenance therapy. Trilege (Agence Nationale de Recherches sur le SIDA 072) Study Team) JAMA. 2000 Jan 12;283(2):205–211. - PubMed
-
- Montaner JS, Reiss P, Cooper D, et al. A randomized, double-blind trial comparing combinations of nevirapine, didanosine, and zidovudine for HIV-infected patients: the INCAS Trial. Italy, The Netherlands, Canada and Australia Study. JAMA. 1998 Mar 25;279(2):930–937. - PubMed
-
- Race E, Dam E, Obry V, Paulous S, Clavel F. Analysis of HIV cross-resistance to protease inhibitors using a rapid single-cycle recombinant virus assay for patients failing on combination therapies. AIDS. 1999 Oct 22;13(15):2061–2068. - PubMed
-
- Harrigan PR, Wynhoven B, Brumme ZL, et al. HIV-1 drug resistance: degree of underestimation by a cross-sectional versus a longitudinal testing approach. J Infect Dis. 2005 Apr 15;191(8):1325–1330. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
