

Lymphomatoid granulomatosis: CT and FDG-PET findings
- PMID: 22043148
- PMCID: PMC3194770
- DOI: 10.3348/kjr.2011.12.6.671
Lymphomatoid granulomatosis: CT and FDG-PET findings
Abstract
Objective: Lymphomatoid granulomatosis (LG) is a rare, aggressive extranodal Epstein-Barr virus (EBV)-positive B-cell lymphoproliferative disease. The purpose of our study was to analyze the CT and fluorodeoxyglucose positron emission tomography (FDG-PET) findings of pulmonary LG.
Materials and methods: Between 2000 and 2009, four patients with pathologically proven pulmonary LG and chest CT were identified. Two of these patients also had FDG-PET. Imaging features of LG on CT and PET were reviewed.
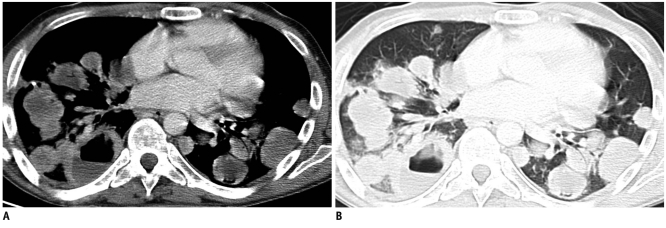
Results: Pulmonary nodules or masses with peribronchovascular, subpleural, and lower lung zonal preponderance were present in all patients. Central low attenuation (4 of 4 patients), ground-glass halo (3 of 4 patients), and peripheral enhancement (4 of 4 patients) were observed in these nodules and masses. An air-bronchogram and cavitation were seen in three of four patients. FDG-PET scans demonstrated avid FDG uptake in the pulmonary nodules and masses.
Conclusion: Pulmonary LG presents with nodules and masses with a lymphatic distribution, as would be expected for a lymphoproliferative disease. However, central low attenuation, ground-glass halo and peripheral enhancement of the nodules/masses are likely related to the angioinvasive nature of this disease. Peripheral enhancement and ground-glass halo, in particular, are valuable characteristic not previously reported that can help radiologists suggest the diagnosis of pulmonary LG.
Keywords: Air-bronchogram sign; Cavitation; Halo sign; Lymphomatoid granulomatosis; Pulmonary masses; Pulmonary nodules.
Figures




Similar articles
-
Pitfall of 18F-FDG PET/CT in Characterization of Relapsed Multisystem Lymphomatoid Granulomatosis.J Nucl Med Technol. 2018 Dec;46(4):396-397. doi: 10.2967/jnmt.118.212274. Epub 2018 Jun 8. J Nucl Med Technol. 2018. PMID: 29884684
-
Pulmonary mucosa-associated lymphoid tissue lymphoma: computed tomography and ¹⁸F fluorodeoxyglucose-positron emission tomography/computed tomography imaging findings and follow-up.J Comput Assist Tomogr. 2011 Sep-Oct;35(5):608-13. doi: 10.1097/RCT.0b013e318227a661. J Comput Assist Tomogr. 2011. PMID: 21926857
-
[A case of lymphomatoid granulomatosis which initially demonstrated a diffuse ground glass appearance].Nihon Kokyuki Gakkai Zasshi. 2010 Jan;48(1):49-54. Nihon Kokyuki Gakkai Zasshi. 2010. PMID: 20163022 Japanese.
-
The Role and Pitfall of F18-FDG PET/CT in Surveillance of High Grade Pulmonary Lymphomatoid Granulomatosis.Curr Probl Diagn Radiol. 2021 May-Jun;50(3):443-449. doi: 10.1067/j.cpradiol.2019.02.002. Epub 2019 Feb 10. Curr Probl Diagn Radiol. 2021. PMID: 30826140 Review.
-
Grade I lymphomatoid granulomatosis with increased uptake of [18F] fluorodeoxyglucose in positron emission tomography: a case report.J Clin Exp Hematop. 2009 May;49(1):39-44. doi: 10.3960/jslrt.49.39. J Clin Exp Hematop. 2009. PMID: 19474516 Review.
Cited by
-
Pulmonary lymphomatoid granulomatosis: An uncommon disease but not to be forgotten-a single centre experience.Respirol Case Rep. 2021 May 26;9(7):e00789. doi: 10.1002/rcr2.789. eCollection 2021 Jul. Respirol Case Rep. 2021. PMID: 34094574 Free PMC article.
-
Primary pulmonary lymphoma: imaging findings in 30 cases.Radiol Med. 2019 Dec;124(12):1262-1269. doi: 10.1007/s11547-019-01091-z. Epub 2019 Oct 3. Radiol Med. 2019. PMID: 31583557
-
Primary Lymphoproliferative Lung Diseases: Imaging and Multidisciplinary Approach.Diagnostics (Basel). 2023 Apr 6;13(7):1360. doi: 10.3390/diagnostics13071360. Diagnostics (Basel). 2023. PMID: 37046580 Free PMC article. Review.
-
An Overview of Selected Rare B-Cell Lymphoproliferative Disorders: Imaging, Histopathologic, and Clinical Features.Cancers (Basel). 2021 Nov 22;13(22):5853. doi: 10.3390/cancers13225853. Cancers (Basel). 2021. PMID: 34831006 Free PMC article. Review.
-
Primary diffuse large B-cell lymphoma or lymphomatoid granulomatosis grade 3: a still-puzzling diagnosis in autopsy.Autops Case Rep. 2013 Dec 31;3(4):29-36. doi: 10.4322/acr.2013.036. eCollection 2013 Oct-Dec. Autops Case Rep. 2013. PMID: 28584804 Free PMC article.
References
-
- Guinee D, Jr, Jaffe E, Kingma D, Fishback N, Wallberg K, Krishnan J, et al. Pulmonary lymphomatoid granulomatosis. Evidence for a proliferation of Epstein-Barr virus infected B-lymphocytes with a prominent T-cell component and vasculitis. Am J Surg Pathol. 1994;18:753–764. - PubMed
-
- Liebow AA, Carrington CR, Friedman PJ. Lymphomatoid granulomatosis. Hum Pathol. 1972;3:457–558. - PubMed
-
- Dee PM, Arora NS, Innes DJ., Jr The pulmonary manifestations of lymphomatoid granulomatosis. Radiology. 1982;143:613–618. - PubMed
-
- Hicken P, Dobie JC, Frew E. The radiology of lymphomatoid granulomatosis in the lung. Clin Radiol. 1979;30:661–664. - PubMed
-
- Wechsler RJ, Steiner RM, Israel HL, Patchefsky AS. Chest radiograph in lymphomatoid granulomatosis: comparison with Wegener granulomatosis. AJR Am J Roentgenol. 1984;142:79–83. - PubMed
