

Short-term and long-term effects of orthopedic biodegradable implants
- PMID: 22043969
- PMCID: PMC3470866
- DOI: 10.1615/jlongtermeffmedimplants.v21.i2.10
Short-term and long-term effects of orthopedic biodegradable implants
Abstract
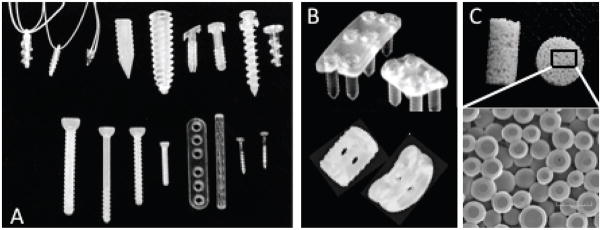
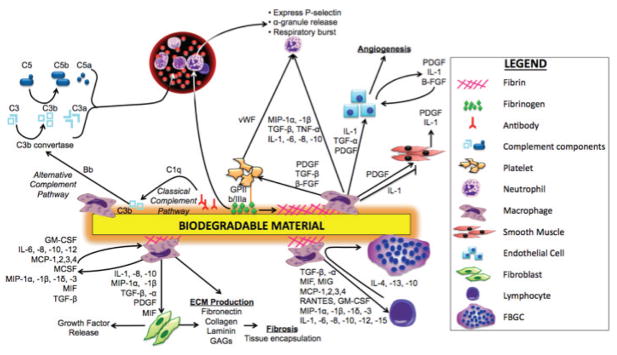
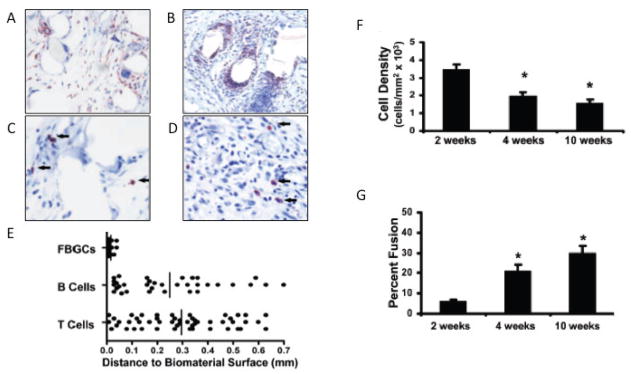
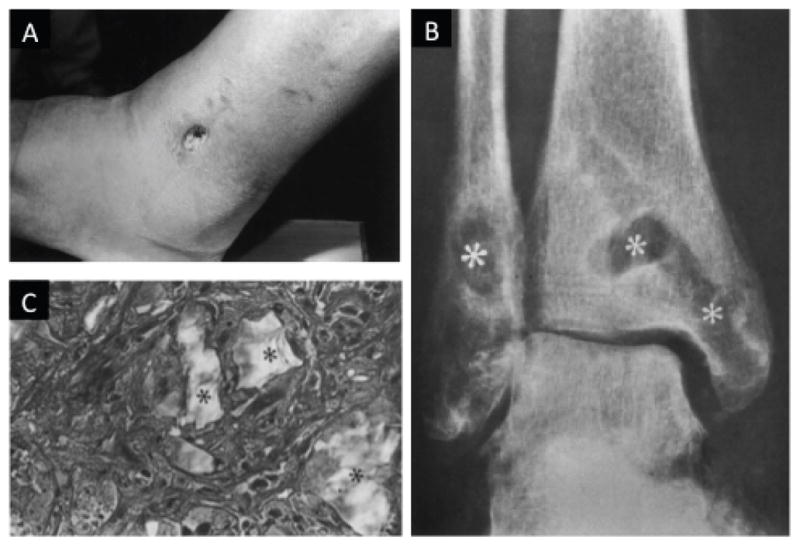
Presently, orthopedic and oral/maxillofacial implants represent a combined $2.8 billion market, a figure expected to experience significant and continued growth. Although traditional permanent implants have been proved clinically efficacious, they are also associated with several drawbacks, including secondary revision and removal surgeries. Non-permanent, biodegradable implants offer a promising alternative for patients, as they provide temporary support and degrade at a rate matching tissue formation, and thus, eliminate the need for secondary surgeries. These implants have been in clinical use for nearly 25 years, competing directly with, or maybe even exceeding, the performance of permanent implants. The initial implantation of biodegradable materials, as with permanent materials, mounts an acute host inflammatory response. Over time, the implant degradation profile and possible degradation product toxicity mediate long-term biodegradable implant-induced inflammation. However, unlike permanent implants, this inflammation is likely to cease once the material disappears. Implant-mediated inflammation is a critical determinant for implant success. Thus, for the development of a proactive biodegradable implant that has the ability to promote optimal bone regeneration and minimal detrimental inflammation, a thorough understanding of short- and long-term inflammatory events is required. Here, we discuss an array of biodegradable orthopedic implants, their associated short- and long- term inflammatory effects, and methods to mediate these inflammatory events.
Figures

References
-
- Mittal R, Morley J, Dinopoulos H, Drakoulakis E, Vermani E, Giannoudis P. Use of bioresorbable implants for stabilisation of distal radius fractures: the United Kingdom patients’ perspective. Injury. 2005 Feb;36(2):333–8. - PubMed
-
- Kulkarni RK, Pani KC, Neuman C, Leonard F. Polylactic acid for surgical implants. Arch Surg. 1966 Nov;93(5):839–43. - PubMed
-
- Rokkanen P, Böstman O, Vainionpää S, Makela EA, Hirvensalo E, Partio EK, Vihtonen K, Pätiälä H, Törmälä P. Absorbable devices in the fixation of fractures. J Trauma. 1996 Mar;40(3 Suppl):S123–7. - PubMed
-
- Rokkanen P, Böstman O, Hirvensalo E, Mäkelä E, Partio E, Pätiälä H, Vainionpää SI, Vihtonen K, Törmälä P. Bioabsorbable fixation in orthopaedic surgery and traumatology. Biomaterials. 2000 Dec;21(24):2607–13. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources