

Mental illness related disparities in diabetes prevalence, quality of care and outcomes: a population-based longitudinal study
- PMID: 22044777
- PMCID: PMC3215928
- DOI: 10.1186/1741-7015-9-118
Mental illness related disparities in diabetes prevalence, quality of care and outcomes: a population-based longitudinal study
Abstract
Background: Health care disparity is a public health challenge. We compared the prevalence of diabetes, quality of care and outcomes between mental health clients (MHCs) and non-MHCs.
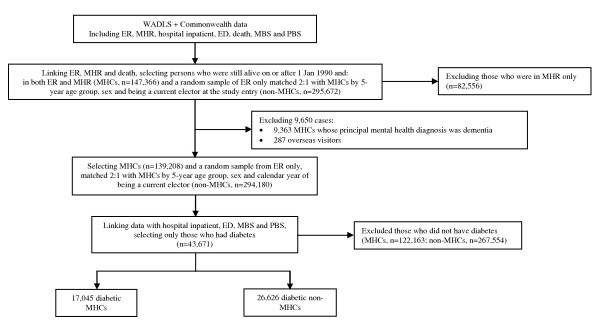
Methods: This was a population-based longitudinal study of 139,208 MHCs and 294,180 matched non-MHCs in Western Australia (WA) from 1990 to 2006, using linked data of mental health registry, electoral roll registrations, hospital admissions, emergency department attendances, deaths, and Medicare and pharmaceutical benefits claims. Diabetes was identified from hospital diagnoses, prescriptions and diabetes-specific primary care claims (17,045 MHCs, 26,626 non-MHCs). Both univariate and multivariate analyses adjusted for socio-demographic factors and case mix were performed to compare the outcome measures among MHCs, category of mental disorders and non-MHCs.
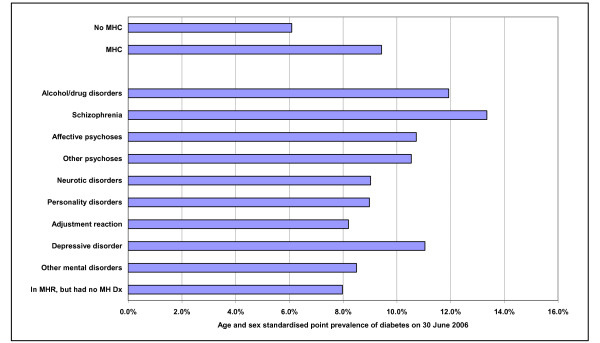
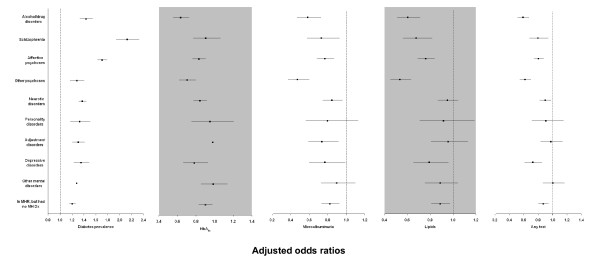
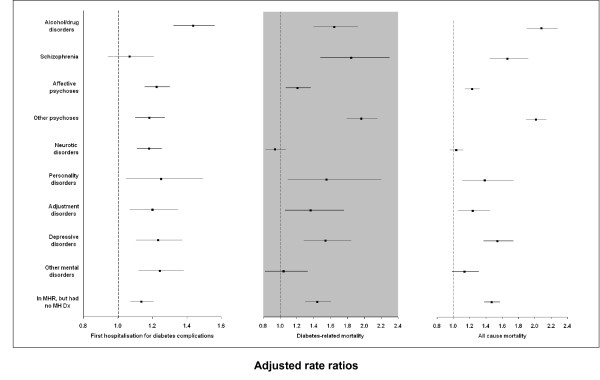
Results: The prevalence of diabetes was significantly higher in MHCs than in non-MHCs (crude age-sex-standardised point-prevalence of diabetes on 30 June 2006 in those aged ≥20 years, 9.3% vs 6.1%, respectively, P < 0.001; adjusted odds ratio (OR) 1.40, 95% CI 1.36 to 1.43). Receipt of recommended pathology tests (HbA1c, microalbuminuria, blood lipids) was suboptimal in both groups, but was lower in MHCs (for all tests combined; adjusted OR 0.81, 95% CI 0.78 to 0.85, at one year; and adjusted rate ratio (RR) 0.86, 95% CI 0.84 to 0.88, during the study period). MHCs also had increased risks of hospitalisation for diabetes complications (adjusted RR 1.20, 95% CI 1.17 to 1.24), diabetes-related mortality (1.43, 1.35 to 1.52) and all-cause mortality (1.47, 1.42 to 1.53). The disparities were most marked for alcohol/drug disorders, schizophrenia, affective disorders, other psychoses and personality disorders.
Conclusions: MHCs warrant special attention for primary and secondary prevention of diabetes, especially at the primary care level.
Figures
References
-
- Lawrence D, Holman CDJ, Jablensky AV. Preventable Physical Illness in People with Mental Illness. Perth: The University of Western Australia; 2001.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
