

Extracellular superoxide dismutase overexpression can reverse the course of hypoxia-induced pulmonary hypertension
- PMID: 22045221
- PMCID: PMC3269642
- DOI: 10.2119/molmed.2011.00339
Extracellular superoxide dismutase overexpression can reverse the course of hypoxia-induced pulmonary hypertension
Abstract
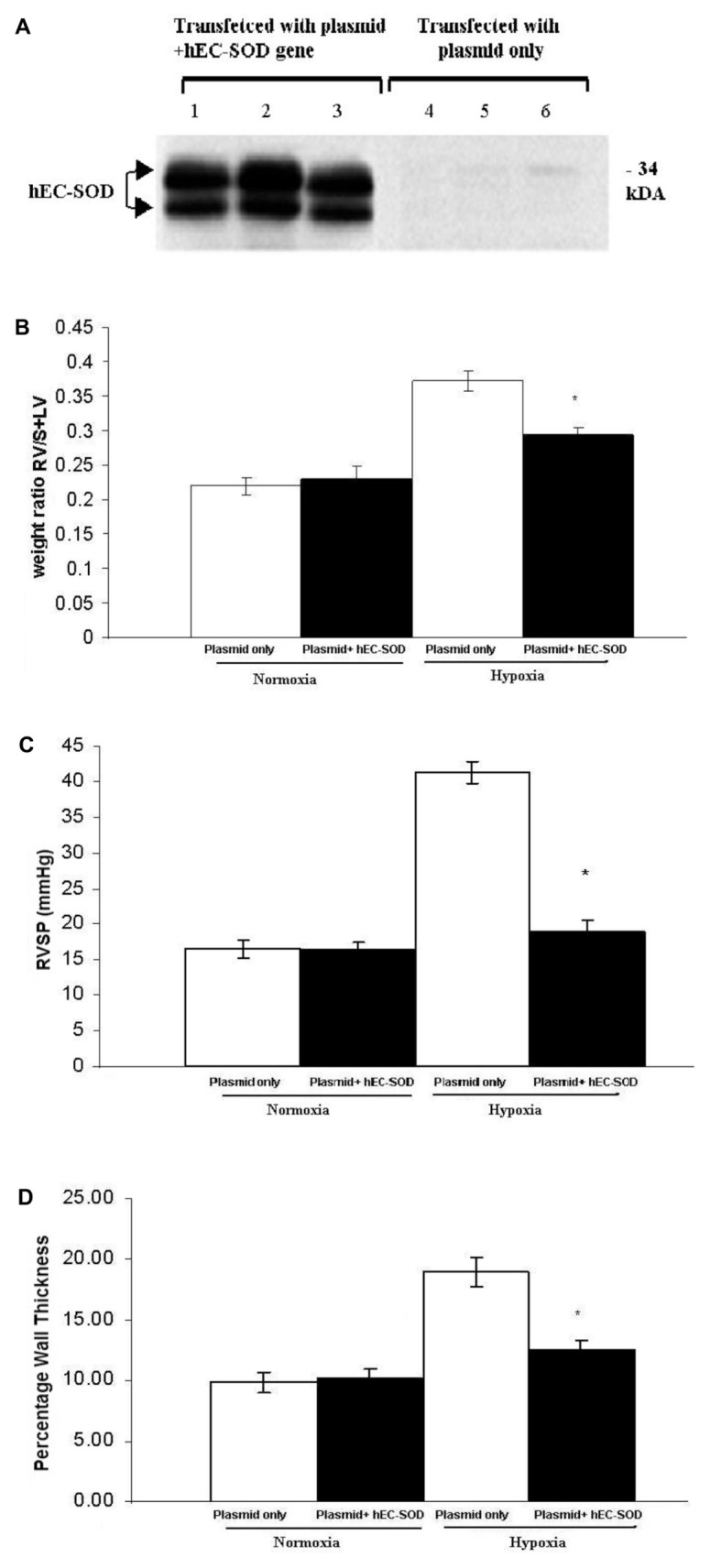
Hypoxia leads to free radical production, which has a pivotal role in the pathophysiology of pulmonary hypertension (PH). We hypothesized that treatment with extracellular superoxide dismutase (EC-SOD) could ameliorate the development of PH induced by hypoxia. In vitro studies using pulmonary microvascular endothelial cells showed that cells transfected with EC-SOD had significantly less accumulation of xanthine oxidase and reactive oxygen species than nontransfected cells after hypoxia exposure for 24 h. To study the prophylactic role of EC-SOD, adult male wild-type (WT) and transgenic (TG) mice, with lung-specific overexpression of human EC-SOD (hEC-SOD), were exposed to fraction of inspired oxygen (FiO(2)) 10% for 10 d. After exposure, right ventricular systolic pressure (RVSP), right ventricular mass (RV/S + LV), pulmonary vascular wall thickness (PVWT) and pulmonary artery contraction/relaxation were assessed. TG mice were protected against PH compared with WT mice with significantly lower RVSP (23.9 ± 1.24 versus 47.2 ± 3.4), RV/S + LV (0.287 ± 0.015 versus 0.335 ± 0.022) and vascular remodeling, indicated by PVWT (14.324 ± 1.107 versus 18.885 ± 1.529). Functional studies using pulmonary arteries isolated from mice indicated that EC-SOD prevents hypoxia-mediated attenuation of nitric oxide-induced relaxation. Therapeutic potential was assessed by exposing WT mice to FiO(2) 10% for 10 d. Half of the group was transfected with plasmid containing cDNA encoding human EC-SOD. The remaining animals were transfected with empty vector. Both groups were exposed to FiO(2) 10% for a further 10 d. Transfected mice had significantly reduced RVSP (18.97 ± 1.12 versus 41.3 ± 1.5), RV/S + LV (0.293 ± 0.012 versus 0.372 ± 0.014) and PVWT (12.51 ± 0.72 versus 18.98 ± 1.24). On the basis of these findings, we concluded that overexpression of EC-SOD prevents the development of PH and ameliorates established PH.
Figures




 , BAL, WBCs count × 1,000;
, BAL, WBCs count × 1,000;
 , BAL, PMNs count × 1,000.
, BAL, PMNs count × 1,000.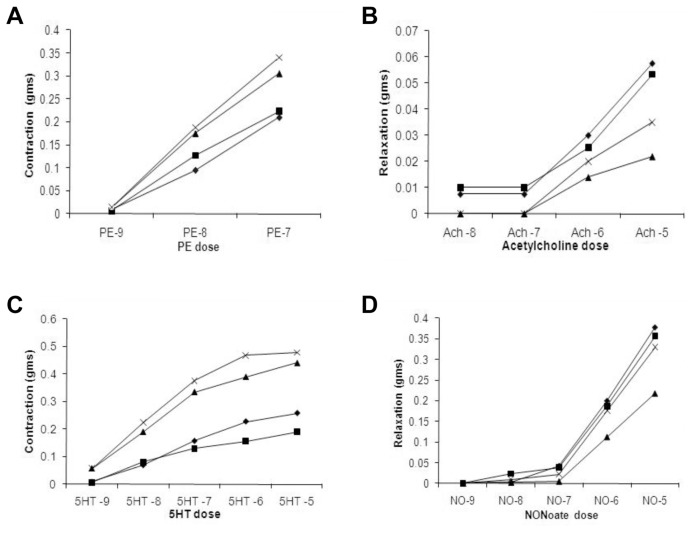
References
-
- Stenmark KR, Fagan KA, Frid MG. Hypoxia-induced pulmonary vascular remodeling: cellular and molecular mechanisms. Circ Res. 2006;99:675–91. - PubMed
-
- Land RD. Neonatal chronic lung disease in the post-surfactant era. Biol Neonate. 2005;88:181–91. - PubMed
-
- Tuder RM, Yun JH, Bhunia A, Fijalkowska I. Hypoxia and chronic lung disease. J Mol Med. 2007;12:1317–24. - PubMed
-
- Lai YL, Wu HD, Chen CF. Antioxidants attenuate chronic hypoxic pulmonary hypertension. J Cardiovasc Pharmacol. 1998;32:714–20. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
