

The pathogenesis and diagnosis of acute kidney injury in multiple myeloma
- PMID: 22045243
- PMCID: PMC3375610
- DOI: 10.1038/nrneph.2011.168
The pathogenesis and diagnosis of acute kidney injury in multiple myeloma
Abstract
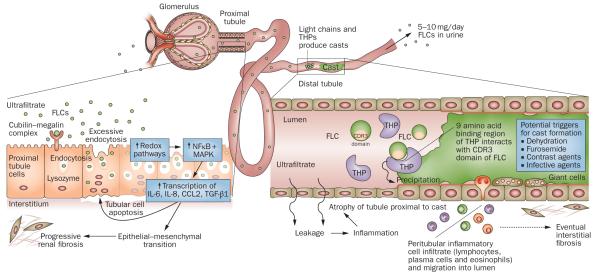
Renal failure remains a principal cause of morbidity for patients with multiple myeloma. Once reversible factors such as hypercalcemia have been corrected, the most common cause of severe renal failure in these patients is a tubulointerstitial pathology that results from the very high circulating concentrations of monoclonal immunoglobulin free light chains. These endogenous proteins can result in isolated proximal tubule cell cytotoxicity, tubulointerstitial nephritis and cast nephropathy (myeloma kidney). Less frequently, high levels of free light chains can lead to immunoglobulin light chain amyloidosis and light chain deposition disease, although these conditions are usually associated with insidious progression of renal failure rather than acute kidney injury. Unless there is rapid intervention, progressive and irreversible damage occurs, particularly interstitial fibrosis and tubular atrophy. Despite advances in our understanding of the pathogenesis of these processes there has been a gap in translating these achievements into improved patient outcomes. The International Kidney and Monoclonal Gammopathy Research Group was formed to address this need. In this Review, we discuss the mechanisms of disease and diagnostic approaches to patients with acute kidney injury complicating multiple myeloma.
Figures
References
-
- Haynes RJ, Read S, Collins GP, Darby SC, Winearls CG. Presentation and survival of patients with severe acute kidney injury and multiple myeloma: a 20-year experience from a single centre. Nephrol. Dial. Transplant. 2010;25:419–426. - PubMed
-
- Bladé J, et al. Renal failure in multiple myeloma: presenting features and predictors of outcome in 94 patients from a single institution. Arch. Intern. Med. 1998;158:1889–1893. - PubMed
-
- Leung N, et al. Improvement of cast nephropathy with plasma exchange depends on the diagnosis and on reduction of serum free light chains. Kidney Int. 2008;73:1282–1288. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
