

Predicting clinical outcomes using baseline and follow-up laboratory data from the hepatitis C long-term treatment against cirrhosis trial
- PMID: 22045670
- PMCID: PMC3718548
- DOI: 10.1002/hep.24550
Predicting clinical outcomes using baseline and follow-up laboratory data from the hepatitis C long-term treatment against cirrhosis trial
Abstract
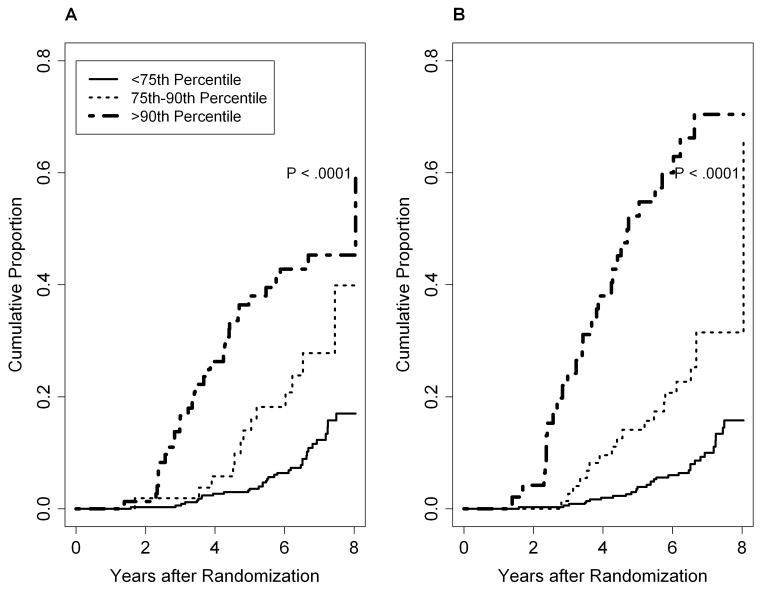
Predicting clinical outcomes in patients with chronic hepatitis C is challenging. We used the hepatitis C long-term treatment against cirrhosis (HALT-C) trial database to develop two models, using baseline values of routinely available laboratory tests together with changes in these values during follow-up to predict clinical decompensation and liver-related death/liver transplant in patients with advanced hepatitis C. Patients randomized to no treatment and who had ≥ 2-year follow-up without a clinical outcome were included in the analysis. Four variables (platelet count, aspartate aminotransferase [AST]/alanine aminotransferase [ALT] ratio, total bilirubin, and albumin) with three categories of change (stable, mild, or severe) over 2 years were analyzed. Cumulative incidence of clinical outcome was determined by Kaplan-Meier analysis and Cox regression was used to evaluate predictors of clinical outcome. In all, 470 patients with 60 events were used to develop models to predict clinical decompensation. Baseline values of all four variables were predictive of decompensation. There was a general trend of increasing outcomes with more marked worsening of laboratory values over 2 years, particularly for patients with abnormal baseline values. A model that included baseline platelet count, AST/ALT ratio, bilirubin, and severe worsening of platelet count, bilirubin, and albumin was the best predictor of clinical decompensation. A total of 483 patients with 79 events were used to evaluate predictors of liver-related death or liver transplant. A model that included baseline platelet count and albumin as well as severe worsening of AST/ALT ratio and albumin was the best predictor of liver-related outcomes.
Conclusion: Both the baseline value and the rapidity in change of the value of routine laboratory variables were shown to be important in predicting clinical outcomes in patients with advanced chronic hepatitis C.
Copyright © 2011 American Association for the Study of Liver Diseases.
Figures




References
-
- Ghany MG, Lok AS, Everhart JE, Everson GT, Lee WM, Curto TM, Wright EC, Stoddard AM, Sterling RK, Di Bisceglie AM, Bonkovsky HL, Morishima C, Morgan TR, Dienstag JL. Predicting clinical and histologic outcomes based on standard laboratory tests in advanced chronic hepatitis C. Gastroenterology. 2010;138:136–46. - PMC - PubMed
-
- Lok AS, Ghany MG, Goodman ZD, Wright EC, Everson GT, Sterling RK, Everhart JE, Lindsay KL, Bonkovsky HL, Di Bisceglie AM, Lee WM, Morgan TR, Dienstag JL, Morishima C. Predicting cirrhosis in patients with hepatitis C based on standard laboratory tests: results of the HALT-C cohort. Hepatology. 2005;42:282–92. - PubMed
-
- Leroy V, Hilleret MN, Sturm N, Trocme C, Renversez JC, Faure P, Morel F, Zarski JP. Prospective comparison of six non-invasive scores for the diagnosis of liver fibrosis in chronic hepatitis C. J Hepatol. 2007;46:775–82. - PubMed
-
- Wai CT, Greenson JK, Fontana RJ, Kalbfleisch JD, Marrero JA, Conjeevaram HS, Lok AS. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology. 2003;38:518–26. - PubMed
-
- Forns X, Ampurdanes S, Llovet JM, Aponte J, Quinto L, Martinez-Bauer E, Bruguera M, Sanchez-Tapias JM, Rodes J. Identification of chronic hepatitis C patients without hepatic fibrosis by a simple predictive model. Hepatology. 2002;36:986–92. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01-DK-9-2325/DK/NIDDK NIH HHS/United States
- 1 UL1 RR024986/RR/NCRR NIH HHS/United States
- N01-DK-9-2321/DK/NIDDK NIH HHS/United States
- 1 UL1 RR024982-01/RR/NCRR NIH HHS/United States
- N01-DK-9-2320/DK/NIDDK NIH HHS/United States
- M01 RR006192/RR/NCRR NIH HHS/United States
- M01 RR001066/RR/NCRR NIH HHS/United States
- M01 RR000633/RR/NCRR NIH HHS/United States
- M01 RR000065/RR/NCRR NIH HHS/United States
- UL1 RR024982/RR/NCRR NIH HHS/United States
- N01-DK-9-2322/DK/NIDDK NIH HHS/United States
- M01 RR000043/RR/NCRR NIH HHS/United States
- N01-DK-9-2323/DK/NIDDK NIH HHS/United States
- M01 RR000827/RR/NCRR NIH HHS/United States
- UL1 RR024986/RR/NCRR NIH HHS/United States
- M01RR-00042/RR/NCRR NIH HHS/United States
- 1 UL1 RR 025780-01/RR/NCRR NIH HHS/United States
- M01RR-00065/RR/NCRR NIH HHS/United States
- N01-DK-9-2328/DK/NIDDK NIH HHS/United States
- N01-DK-9-2318/DK/NIDDK NIH HHS/United States
- N01-DK-9-2324/DK/NIDDK NIH HHS/United States
- N01-DK-9-2319/DK/NIDDK NIH HHS/United States
- M01RR-00051/RR/NCRR NIH HHS/United States
- UL1 RR025780/RR/NCRR NIH HHS/United States
- 1 UL1 RR025758-01/RR/NCRR NIH HHS/United States
- ZIA DK075009/ImNIH/Intramural NIH HHS/United States
- M01RR-00827/RR/NCRR NIH HHS/United States
- N01-DK-9-2327/DK/NIDDK NIH HHS/United States
- M01RR-01066/RR/NCRR NIH HHS/United States
- M01 RR000051/RR/NCRR NIH HHS/United States
- N01-DK-9-2326/DK/NIDDK NIH HHS/United States
- UL1 RR025758/RR/NCRR NIH HHS/United States
- M01 RR000042/RR/NCRR NIH HHS/United States
- M01RR-00633/RR/NCRR NIH HHS/United States
- M01RR-00043/RR/NCRR NIH HHS/United States
- M01RR-06192/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases