

Long-term outcomes among older patients following nonmyeloablative conditioning and allogeneic hematopoietic cell transplantation for advanced hematologic malignancies
- PMID: 22045765
- PMCID: PMC3217787
- DOI: 10.1001/jama.2011.1558
Long-term outcomes among older patients following nonmyeloablative conditioning and allogeneic hematopoietic cell transplantation for advanced hematologic malignancies
Abstract
Context: A minimally toxic nonmyeloablative regimen was developed for allogeneic hematopoietic cell transplantation (HCT) to treat patients with advanced hematologic malignancies who are older or have comorbid conditions.
Objective: To describe outcomes of patients 60 years or older after receiving minimally toxic nonmyeloablative allogeneic HCT.
Design, setting, and participants: From 1998 to 2008, 372 patients aged 60 to 75 years were enrolled in prospective clinical HCT trials at 18 collaborating institutions using conditioning with low-dose total body irradiation alone or combined with fludarabine, 90 mg/m(2), before related (n = 184) or unrelated (n = 188) donor transplants. Postgrafting immunosuppression included mycophenolate mofetil and a calcineurin inhibitor.
Main outcome measures: Overall and progression-free survival were estimated by Kaplan-Meier method. Cumulative incidence estimates were calculated for acute and chronic graft-vs-host disease, toxicities, achievement of full donor chimerism, complete remission, relapse, and nonrelapse mortality. Hazard ratios (HRs) were estimated from Cox regression models.
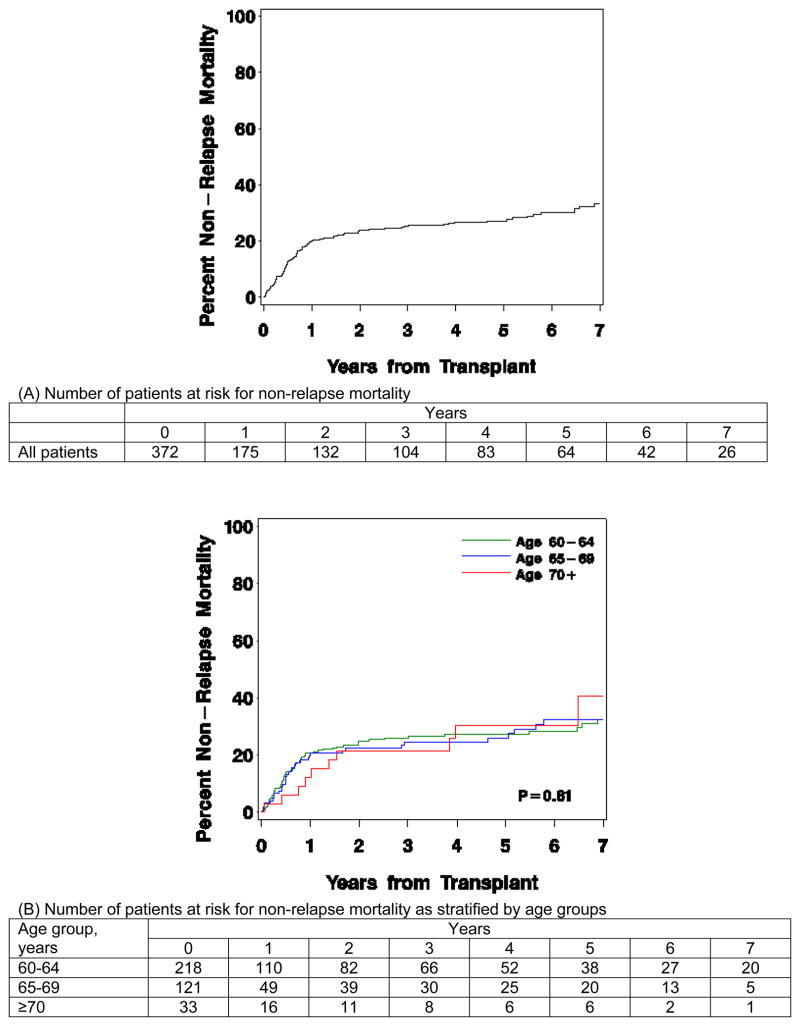
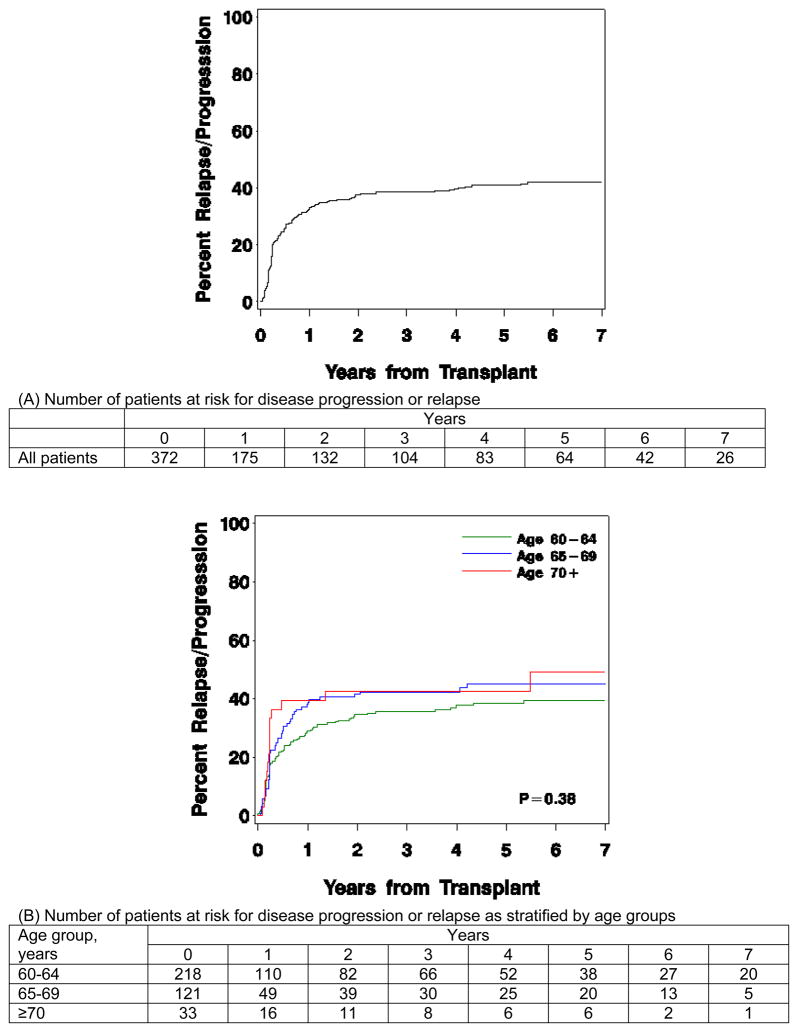
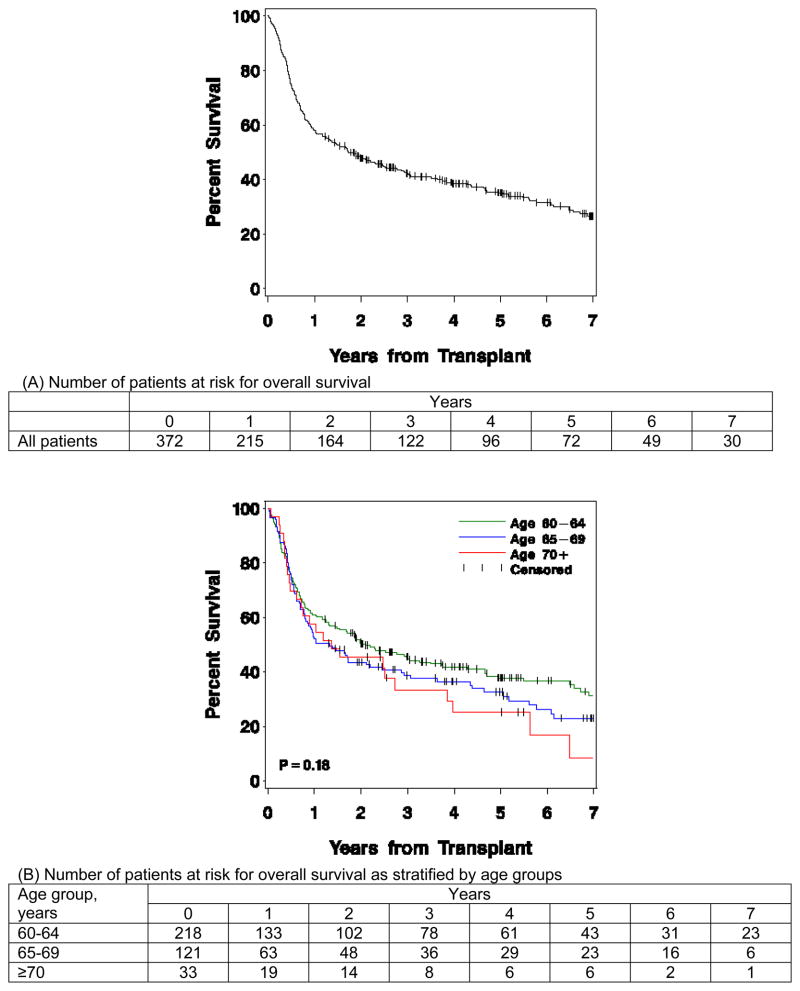
Results: Overall, 5-year cumulative incidences of nonrelapse mortality and relapse were 27% (95% CI, 22%-32%) and 41% (95% CI, 36%-46%), respectively, leading to 5-year overall and progression-free survival of 35% (95% CI, 30%-40%) and 32% (95% CI, 27%-37%), respectively. These outcomes were not statistically significantly different when stratified by age groups. Furthermore, increasing age was not associated with increases in acute or chronic graft-vs-host disease or organ toxicities. In multivariate models, HCT-specific comorbidity index scores of 1 to 2 (HR, 1.58 [95% CI, 1.08-2.31]) and 3 or greater (HR, 1.97 [95% CI, 1.38-2.80]) were associated with worse survival compared with an HCT-specific comorbidity index score of 0 (P = .003 overall). Similarly, standard relapse risk (HR, 1.67 [95% CI, 1.10-2.54]) and high relapse risk (HR, 2.22 [95% CI, 1.43-3.43]) were associated with worse survival compared with low relapse risk (P < .001 overall).
Conclusion: Among patients aged 60 to 75 years treated with nonmyeloablative allogeneic HCT, 5-year overall and progression-free survivals were 35% and 32%, respectively.
Conflict of interest statement
Figures
Comment in
-
Overcoming the age barrier in hematopoietic stem cell transplantation: progress, but still a long way to go.JAMA. 2011 Nov 2;306(17):1918-20. doi: 10.1001/jama.2011.1612. JAMA. 2011. PMID: 22045771 No abstract available.
-
Are reduced-intensity transplants safe in older patients with hematologic malignancies?Expert Rev Hematol. 2012 Apr;5(2):149-52. doi: 10.1586/ehm.12.9. Expert Rev Hematol. 2012. PMID: 22475283
References
-
- Gratwohl A, Hermans J, Goldman JM, et al. Risk assessment for patients with chronic myeloid leukaemia before allogeneic blood or marrow transplantation. Lancet. 1998;352(9134):1087–1092. - PubMed
-
- SEER Cancer Statistics Review, 1975–2007. Bethesda, MD: National Cancer Institute; 2010. http://seer.cancer.gov/csr/1975_2007/, based on November 2009 SEER data submission, posted to the SEER web site.
-
- United States Cancer Statistics: 1999–2005 Incidence, WONDER Online Database. United States Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute; 2008. http://wonder.cdc.gov/cancer-v2005.html.
-
- McSweeney PA, Niederwieser D, Shizuru JA, et al. Hematopoietic cell transplantation in older patients with hematologic malignancies: replacing high-dose cytotoxic therapy with graft-versus-tumor effects. Blood. 2001;97(11):3390–3400. - PubMed
-
- Maris MB, Niederwieser D, Sandmaier BM, et al. HLA-matched unrelated donor hematopoietic cell transplantation after nonmyeloablative conditioning for patients with hematologic malignancies. Blood. 2003;102(6):2021–2030. - PubMed
