

Spectrum of cancer risk among US solid organ transplant recipients
- PMID: 22045767
- PMCID: PMC3310893
- DOI: 10.1001/jama.2011.1592
Spectrum of cancer risk among US solid organ transplant recipients
Abstract
Context: Solid organ transplant recipients have elevated cancer risk due to immunosuppression and oncogenic viral infections. Because most prior research has concerned kidney recipients, large studies that include recipients of differing organs can inform cancer etiology.
Objective: To describe the overall pattern of cancer following solid organ transplantation.
Design, setting, and participants: Cohort study using linked data on solid organ transplant recipients from the US Scientific Registry of Transplant Recipients (1987-2008) and 13 state and regional cancer registries.
Main outcome measures: Standardized incidence ratios (SIRs) and excess absolute risks (EARs) assessing relative and absolute cancer risk in transplant recipients compared with the general population.
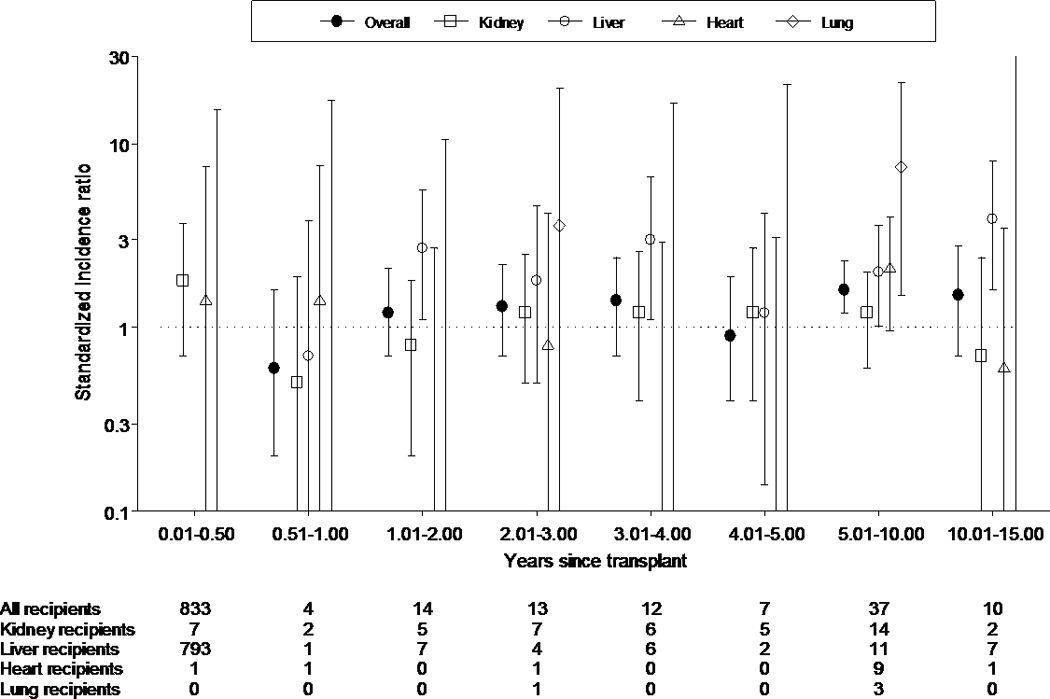
Results: The registry linkages yielded data on 175,732 solid organ transplants (58.4% for kidney, 21.6% for liver, 10.0% for heart, and 4.0% for lung). The overall cancer risk was elevated with 10,656 cases and an incidence of 1375 per 100,000 person-years (SIR, 2.10 [95% CI, 2.06-2.14]; EAR, 719.3 [95% CI, 693.3-745.6] per 100,000 person-years). Risk was increased for 32 different malignancies, some related to known infections (eg, anal cancer, Kaposi sarcoma) and others unrelated (eg, melanoma, thyroid and lip cancers). The most common malignancies with elevated risk were non-Hodgkin lymphoma (n = 1504; incidence: 194.0 per 100,000 person-years; SIR, 7.54 [95% CI, 7.17-7.93]; EAR, 168.3 [95% CI, 158.6-178.4] per 100,000 person-years) and cancers of the lung (n = 1344; incidence: 173.4 per 100,000 person-years; SIR, 1.97 [95% CI, 1.86-2.08]; EAR, 85.3 [95% CI, 76.2-94.8] per 100,000 person-years), liver (n = 930; incidence: 120.0 per 100,000 person-years; SIR, 11.56 [95% CI, 10.83-12.33]; EAR, 109.6 [95% CI, 102.0-117.6] per 100,000 person-years), and kidney (n = 752; incidence: 97.0 per 100,000 person-years; SIR, 4.65 [95% CI, 4.32-4.99]; EAR, 76.1 [95% CI, 69.3-83.3] per 100,000 person-years). Lung cancer risk was most elevated in lung recipients (SIR, 6.13 [95% CI, 5.18-7.21]) but also increased among other recipients (kidney: SIR, 1.46 [95% CI, 1.34-1.59]; liver: SIR, 1.95 [95% CI, 1.74-2.19]; and heart: SIR, 2.67 [95% CI, 2.40-2.95]). Liver cancer risk was elevated only among liver recipients (SIR, 43.83 [95% CI, 40.90-46.91]), who manifested exceptional risk in the first 6 months (SIR, 508.97 [95% CI, 474.16-545.66]) and a 2-fold excess risk for 10 to 15 years thereafter (SIR, 2.22 [95% CI, 1.57-3.04]). Among kidney recipients, kidney cancer risk was elevated (SIR, 6.66 [95% CI, 6.12-7.23]) and bimodal in onset time. Kidney cancer risk also was increased in liver recipients (SIR, 1.80 [95% CI, 1.40-2.29]) and heart recipients (SIR, 2.90 [95% CI, 2.32-3.59]).
Conclusion: Compared with the general population, recipients of a kidney, liver, heart, or lung transplant have an increased risk for diverse infection-related and unrelated cancers.
Conflict of interest statement
Conflict of Interest Disclosures: All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Bertram L. Kasiske reported that he receives grant funding from BMS. Ajay K. Israni reported that he receives grant funding Bristol-Myers Squibb, Roche, and Genzyme. Jon J. Snyder reported that he receives consultancy fees and research support from Genzyme, research support from Bristol-Myers Squibb, and payment for development of educational presentations from the American Society of Nephrology. No other disclosures were reported.
Figures



Comment in
-
Cancer risk after organ transplantation.JAMA. 2012 Feb 15;307(7):663; author reply 663-4. doi: 10.1001/jama.2012.140. JAMA. 2012. PMID: 22337671 No abstract available.
References
-
- Organ Procurement and Transplantation Network. http://optn.transplant.hrsa.gov/. 5-5-2011.
-
- Vajdic CM, van Leeuwen MT. Cancer incidence and risk factors after solid organ transplantation. Int J Cancer. 2009;125:1747–1754. - PubMed
-
- Birkeland SA, Storm HH, Lamm LU, Barlow L, Blohme I, Forsberg B, et al. Cancer risk after renal transplantation in the Nordic countries, 1964–1986. Int J Cancer. 1995;60:183–189. - PubMed
-
- Collett D, Mumford L, Banner NR, Neuberger J, Watson C. Comparison of the incidence of malignancy in recipients of different types of organ: a UK Registry audit. Am J Transplant. 2010;10:1889–1896. - PubMed
-
- Villeneuve PJ, Schaubel DE, Fenton SS, Shepherd FA, Jiang Y, Mao Y. Cancer incidence among Canadian kidney transplant recipients. Am J Transplant. 2007;7:941–948. - PubMed
Publication types
MeSH terms
Grants and funding
- N01-PC-54405/PC/NCI NIH HHS/United States
- 5U58DP000812-03/DP/NCCDPHP CDC HHS/United States
- U58 DP000848-04/DP/NCCDPHP CDC HHS/United States
- HHSN261201000036C/CA/NCI NIH HHS/United States
- 5U58DP000817-05/DP/NCCDPHP CDC HHS/United States
- U58 DP000807/DP/NCCDPHP CDC HHS/United States
- N01 PC035142/CA/NCI NIH HHS/United States
- N01 PC054405/CA/NCI NIH HHS/United States
- HHSN261201000035I/CA/NCI NIH HHS/United States
- U58 DP000832/DP/NCCDPHP CDC HHS/United States
- HHSN261201000037C/CA/NCI NIH HHS/United States
- 5U58DP000824-04/DP/NCCDPHP CDC HHS/United States
- N01-PC-35142/PC/NCI NIH HHS/United States
- U58 DP000805/DP/NCCDPHP CDC HHS/United States
- U58 DP000817/DP/NCCDPHP CDC HHS/United States
- 5658DP000805-04/DP/NCCDPHP CDC HHS/United States
- N01-PC-35137/PC/NCI NIH HHS/United States
- N01 PC035143/CA/NCI NIH HHS/United States
- N01-PC-35139/PC/NCI NIH HHS/United States
- U58DP000832/DP/NCCDPHP CDC HHS/United States
- N01 PC035139/CA/NCI NIH HHS/United States
- 5U58/DP000808-03/DP/NCCDPHP CDC HHS/United States
- ZIA CP010150/ImNIH/Intramural NIH HHS/United States
- N01 PC035137/CA/NCI NIH HHS/United States
- 1U58 DP000807-01/DP/NCCDPHP CDC HHS/United States
- U58 DP000808/DP/NCCDPHP CDC HHS/United States
- U58 DP000848/DP/NCCDPHP CDC HHS/United States
- U58 DP000812/DP/NCCDPHP CDC HHS/United States
- HHSN261201000024C/CA/NCI NIH HHS/United States
- HHSN261201000035C/PC/NCI NIH HHS/United States
- HHSN261201000034C/CA/NCI NIH HHS/United States
- N01-PC-35143/PC/NCI NIH HHS/United States
- U58 DP000824/DP/NCCDPHP CDC HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
