

Physiological phenomenology of neurally-mediated syncope with management implications
- PMID: 22046292
- PMCID: PMC3201957
- DOI: 10.1371/journal.pone.0026489
Physiological phenomenology of neurally-mediated syncope with management implications
Abstract
Background: Due to lack of efficacy in recent trials, current guidelines for the treatment of neurally-mediated (vasovagal) syncope do not promote cardiac pacemaker implantation. However, the finding of asystole during head-up tilt -induced (pre)syncope may lead to excessive cardioinhibitory syncope diagnosis and treatment with cardiac pacemakers as blood pressure is often discontinuously measured. Furthermore, physicians may be more inclined to implant cardiac pacemakers in older patients. We hypothesized that true cardioinhibitory syncope in which the decrease in heart rate precedes the fall in blood pressure is a very rare finding which might explain the lack of efficacy of pacemakers in neurally-mediated syncope.
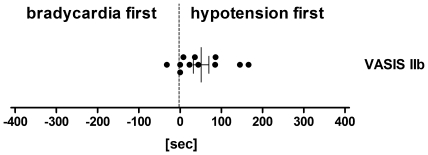
Methods: We studied 173 consecutive patients referred for unexplained syncope (114 women, 59 men, 42 ± 1 years, 17 ± 2 syncopal episodes). All had experienced (pre)syncope during head-up tilt testing followed by additional lower body negative suction. We classified hemodynamic responses according to the modified Vasovagal Syncope International Study (VASIS) classification as mixed response (VASIS I), cardioinhibitory without (VASIS IIa) or with asystole (VASIS IIb), and vasodepressor (VASIS III). Then, we defined the exact temporal relationship between hypotension and bradycardia to identify patients with true cardioinhibitory syncope.
Results: Of the (pre)syncopal events during tilt testing, 63% were classified as VASIS I, 6% as VASIS IIb, 2% as VASIS IIa, and 29% as VASIS III. Cardioinhibitory responses (VASIS class II) progressively decreased from the youngest to the oldest age quartile. With more detailed temporal analysis, blood pressure reduction preceded the heart-rate decrease in all but six individuals (97%) overall and in 10 out of 11 patients with asystole (VASIS IIb).
Conclusions: Hypotension precedes bradycardia onset during head-up tilt-induced (pre)syncope in the vast majority of patients, even in those classified as cardioinhibitory syncope according to the modified VASIS classification. Furthermore, cardioinhibitory syncope becomes less frequent with increasing age.
Conflict of interest statement
Figures




References
-
- Parry SW, Tan MP. An approach to the evaluation and management of syncope in adults. BMJ. 2010;340 - PubMed
-
- Romme J, van Dijk N, Boer K, Dekker L, Stam J, et al. Influence of age and gender on the occurrence and presentation of reflex syncope. Clinical Autonomic Research. 2008;18:127–133. - PubMed
-
- Rose MS, Koshman ML, Ritchie D, Sheldon R. The development and preliminary validation of a scale measuring the impact of syncope on quality of life. Europace. 2009;11:1369–1374. - PubMed
-
- Mosqueda-Garcia R, Furlan R, Tank J, Fernandez-Violante R. The elusive pathophysiology of neurally mediated syncope. Circulation. 2000;102:2898–2906. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
