

The Alzheimer's Disease Neuroimaging Initiative: a review of papers published since its inception
- PMID: 22047634
- PMCID: PMC3329969
- DOI: 10.1016/j.jalz.2011.09.172
The Alzheimer's Disease Neuroimaging Initiative: a review of papers published since its inception
Abstract
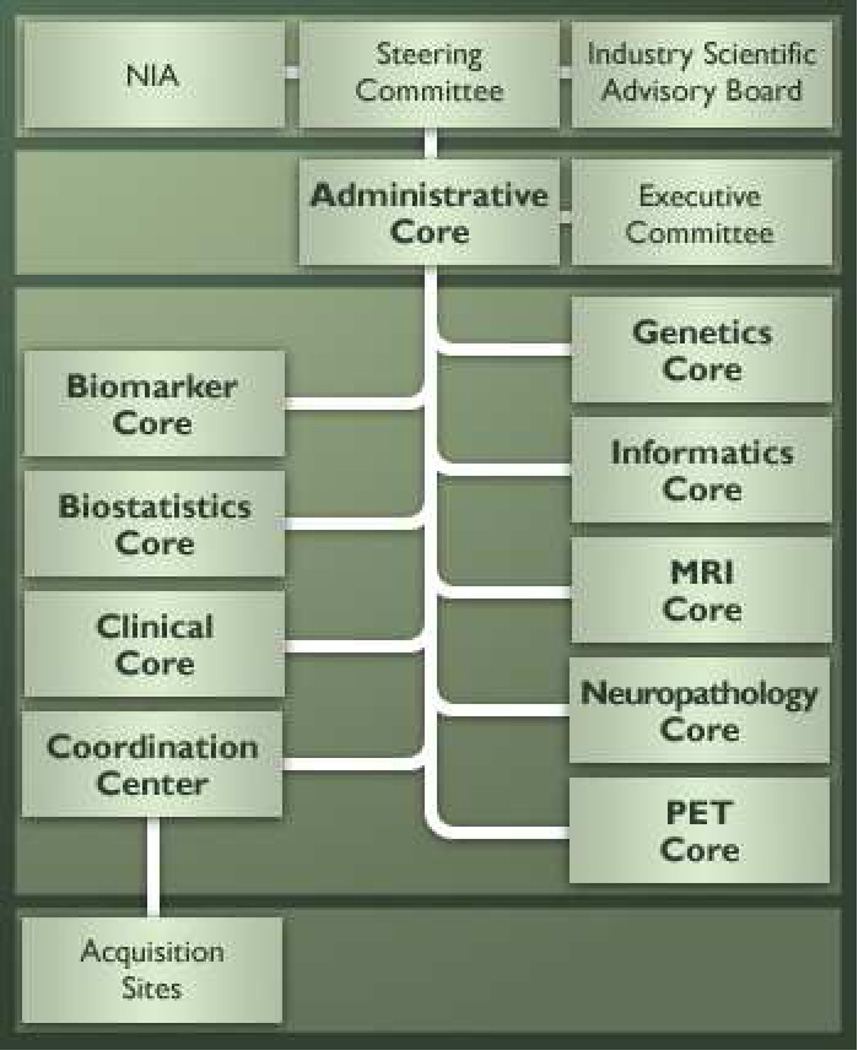
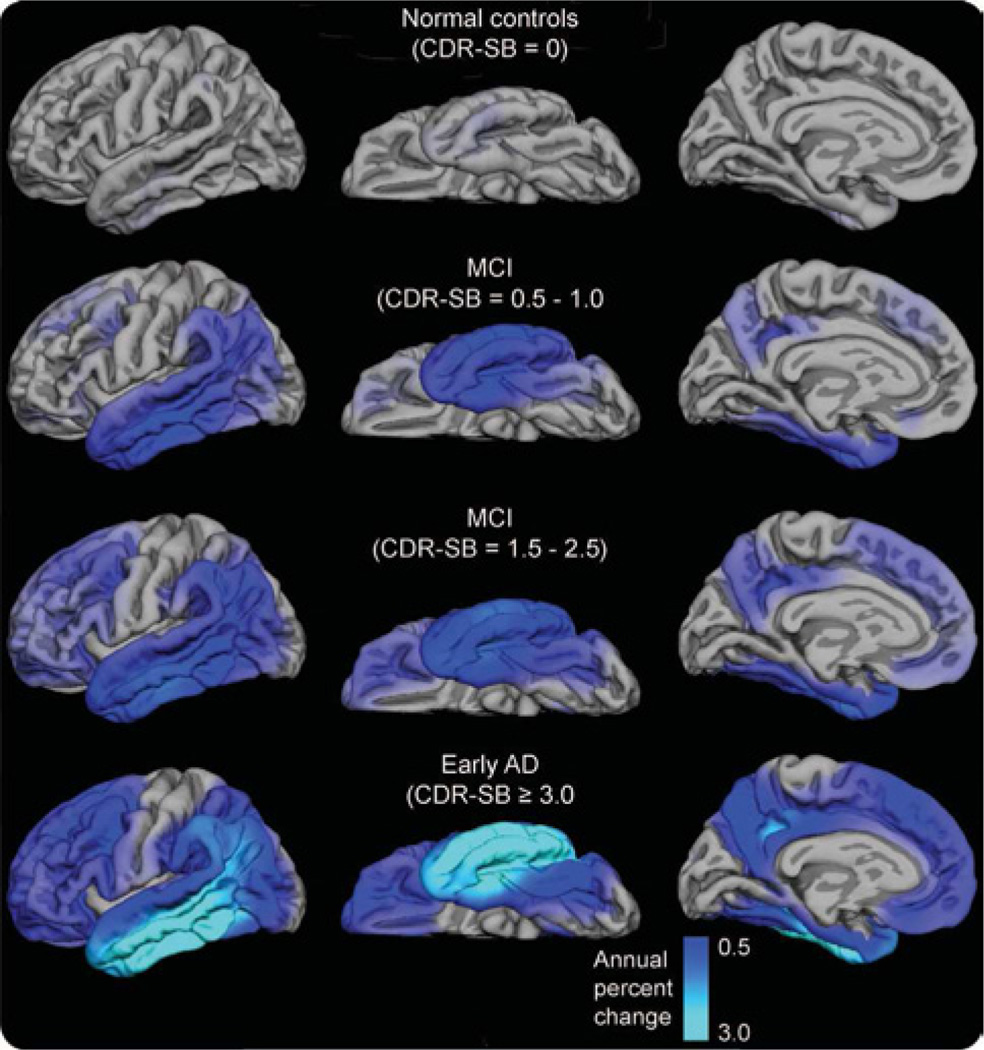
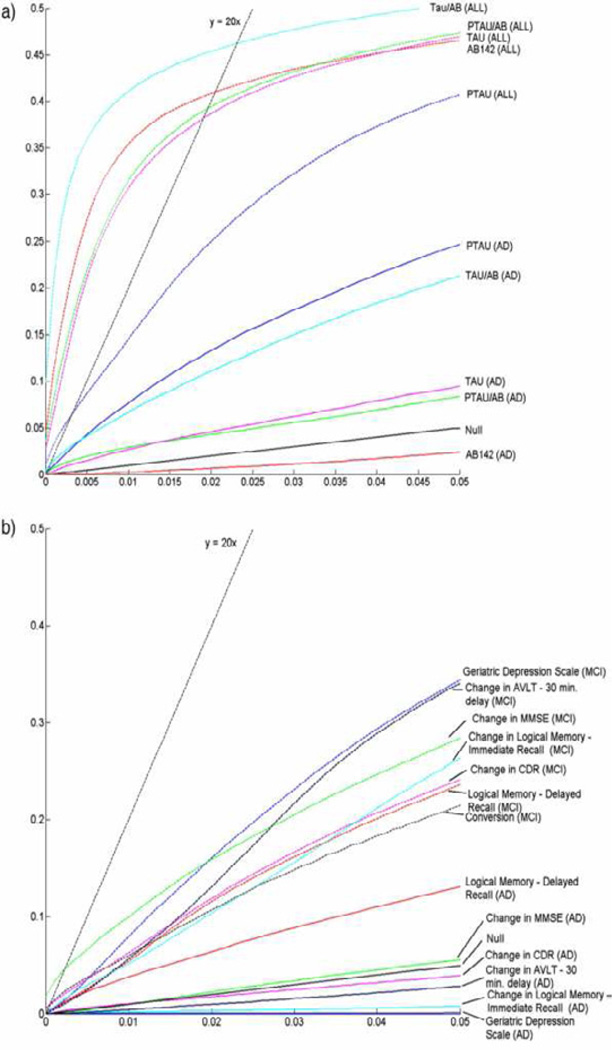
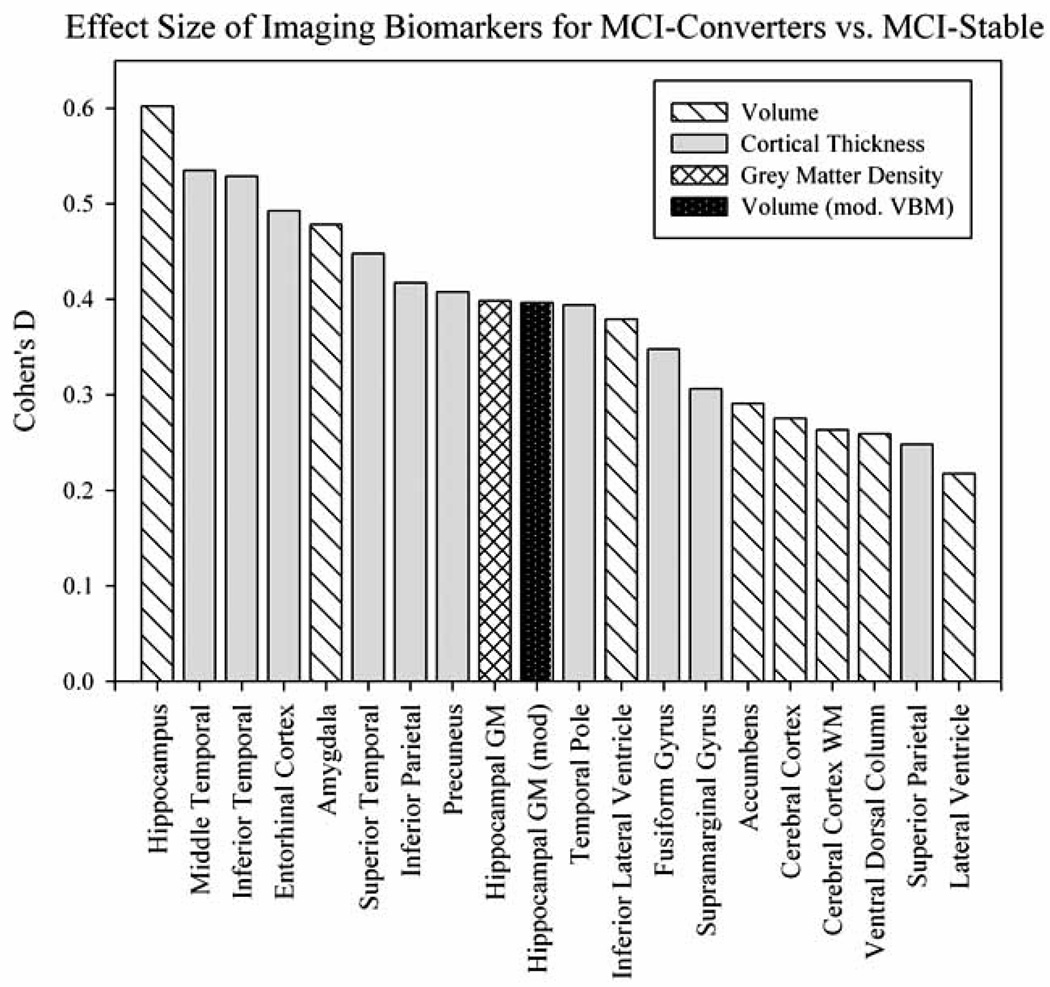
The Alzheimer's Disease Neuroimaging Initiative (ADNI) is an ongoing, longitudinal, multicenter study designed to develop clinical, imaging, genetic, and biochemical biomarkers for the early detection and tracking of Alzheimer's disease (AD). The study aimed to enroll 400 subjects with early mild cognitive impairment (MCI), 200 subjects with early AD, and 200 normal control subjects; $67 million funding was provided by both the public and private sectors, including the National Institute on Aging, 13 pharmaceutical companies, and 2 foundations that provided support through the Foundation for the National Institutes of Health. This article reviews all papers published since the inception of the initiative and summarizes the results as of February 2011. The major accomplishments of ADNI have been as follows: (1) the development of standardized methods for clinical tests, magnetic resonance imaging (MRI), positron emission tomography (PET), and cerebrospinal fluid (CSF) biomarkers in a multicenter setting; (2) elucidation of the patterns and rates of change of imaging and CSF biomarker measurements in control subjects, MCI patients, and AD patients. CSF biomarkers are consistent with disease trajectories predicted by β-amyloid cascade (Hardy, J Alzheimers Dis 2006;9(Suppl 3):151-3) and tau-mediated neurodegeneration hypotheses for AD, whereas brain atrophy and hypometabolism levels show predicted patterns but exhibit differing rates of change depending on region and disease severity; (3) the assessment of alternative methods of diagnostic categorization. Currently, the best classifiers combine optimum features from multiple modalities, including MRI, [(18)F]-fluorodeoxyglucose-PET, CSF biomarkers, and clinical tests; (4) the development of methods for the early detection of AD. CSF biomarkers, β-amyloid 42 and tau, as well as amyloid PET may reflect the earliest steps in AD pathology in mildly symptomatic or even nonsymptomatic subjects, and are leading candidates for the detection of AD in its preclinical stages; (5) the improvement of clinical trial efficiency through the identification of subjects most likely to undergo imminent future clinical decline and the use of more sensitive outcome measures to reduce sample sizes. Baseline cognitive and/or MRI measures generally predicted future decline better than other modalities, whereas MRI measures of change were shown to be the most efficient outcome measures; (6) the confirmation of the AD risk loci CLU, CR1, and PICALM and the identification of novel candidate risk loci; (7) worldwide impact through the establishment of ADNI-like programs in Europe, Asia, and Australia; (8) understanding the biology and pathobiology of normal aging, MCI, and AD through integration of ADNI biomarker data with clinical data from ADNI to stimulate research that will resolve controversies about competing hypotheses on the etiopathogenesis of AD, thereby advancing efforts to find disease-modifying drugs for AD; and (9) the establishment of infrastructure to allow sharing of all raw and processed data without embargo to interested scientific investigators throughout the world. The ADNI study was extended by a 2-year Grand Opportunities grant in 2009 and a renewal of ADNI (ADNI-2) in October 2010 through to 2016, with enrollment of an additional 550 participants.
Published by Elsevier Inc.
Figures





















References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
