

Cerebrovascular disease, β-amyloid, and cognition in aging
- PMID: 22048124
- PMCID: PMC3274647
- DOI: 10.1016/j.neurobiolaging.2011.10.001
Cerebrovascular disease, β-amyloid, and cognition in aging
Abstract
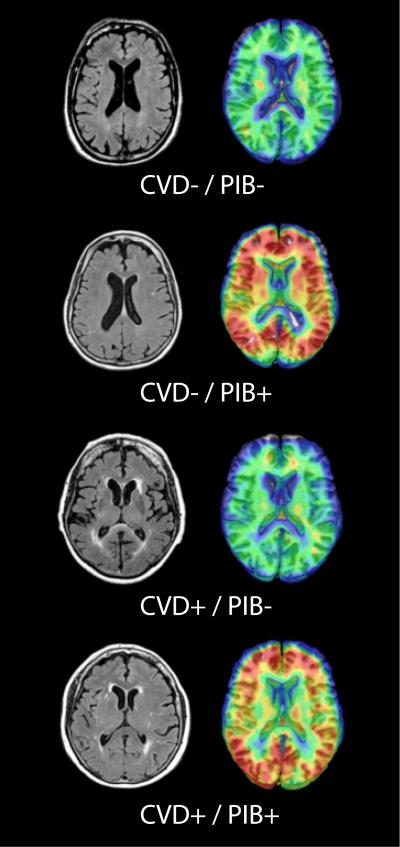
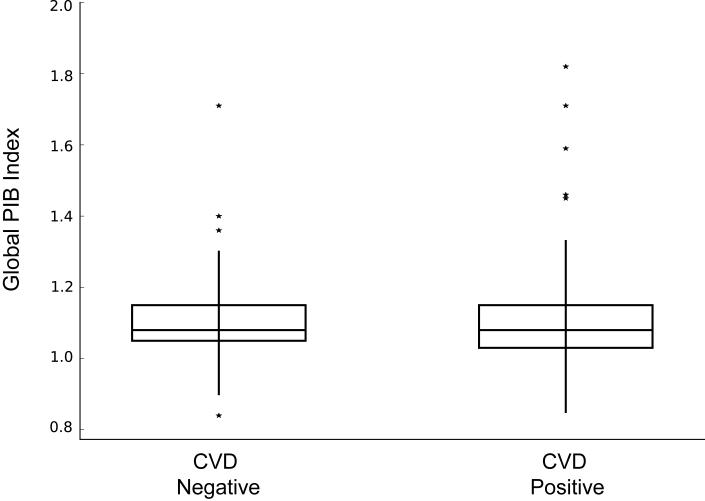
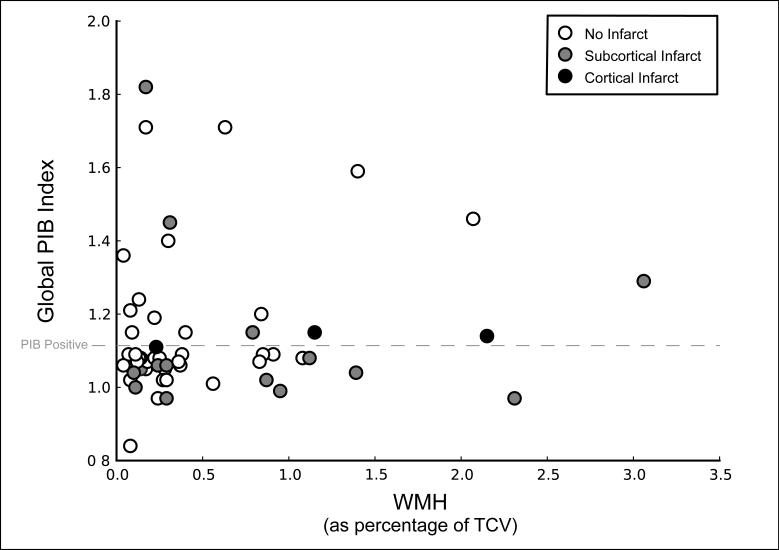
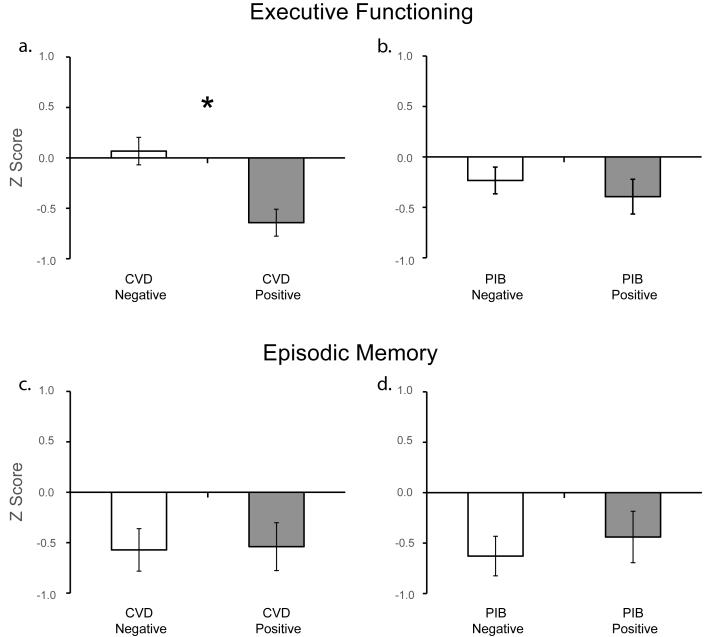
The present study evaluated cerebrovascular disease (CVD), β-amyloid (Aβ), and cognition in clinically normal elderly adults. Fifty-four participants underwent magnetic resonance imaging (MRI), Pittsburgh compound B (PIB)-positron emission tomography (PET) imaging, and neuropsychological evaluation. High white matter hyperintensity burden and/or presence of infarct defined CVD status (CVD-: n = 27; CVD+: n = 27). PIB-positron emission tomography ratios of Aβ deposition were extracted using Logan plotting (cerebellar reference). Presence of high levels of Aβ in prespecified regions determined PIB status (PIB-: n = 33; PIB+: n = 21). Executive functioning and episodic memory were measured using composite scales. CVD and Aβ, defined as dichotomous or continuous variables, were unrelated to one another. CVD+ participants showed lower executive functioning (p = 0.001) when compared with CVD- individuals. Neither PIB status nor amount of Aβ affected cognition (ps ≥ 0.45), and there was no statistical interaction between CVD and PIB on either cognitive measure. Within this spectrum of normal aging CVD and Aβ aggregation appear to be independent processes with CVD primarily affecting cognition.
Copyright © 2012 Elsevier Inc. All rights reserved.
Figures
References
-
- Aizenstein HJ, Nebes RD, Saxton JA, Price JC, Mathis CA, Tsopelas ND, Ziolko SK, James JA, Snitz BE, Houck PR, Bi W, Cohen AD, Lopresti BJ, DeKosky ST, Halligan EM, Klunk WE. Frequent amyloid deposition without significant cognitive impairment among the elderly. Arch Neurol. 2008;65(11):1509–17. - PMC - PubMed
-
- Benisty S, Gouw AA, Porcher R, Madureira S, Hernandez K, Poggesi A, van der Flier WM, Van Straaten EC, Verdelho A, Ferro J, Pantoni L, Inzitari D, Barkhof F, Fazekas F, Chabriat H. Location of lacunar infarcts correlates with cognition in a sample of non-disabled subjects with age-related white-matter changes: the LADIS study. J Neurol Neurosurg Psychiatry. 2009;80(5):478–83. - PubMed
-
- Bennett DA, Schneider JA, Arvanitakis Z, Kelly JF, Aggarwal NT, Shah RC, Wilson RS. Neuropathology of older persons without cognitive impairment from two community-based studies. Neurology. 2006;66(12):1837–44. - PubMed
-
- Bernick C, Kuller L, Dulberg C, Longstreth WT, Jr., Manolio T, Beauchamp N, Price T. Silent MRI infarcts and the risk of future stroke: the cardiovascular health study. Neurology. 2001;57(7):1222–9. - PubMed
-
- Breteler MM. Vascular risk factors for Alzheimer’s disease: an epidemiologic perspective. Neurobiol Aging. 2000;21(2):153–60. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
