

Phase II, open-label, randomized trial of the MEK1/2 inhibitor selumetinib as monotherapy versus temozolomide in patients with advanced melanoma
- PMID: 22048237
- PMCID: PMC3549298
- DOI: 10.1158/1078-0432.CCR-11-1491
Phase II, open-label, randomized trial of the MEK1/2 inhibitor selumetinib as monotherapy versus temozolomide in patients with advanced melanoma
Abstract
Purpose: To compare the efficacy and tolerability of the mitogen-activated protein (MAP)/extracellular signal-regulated (ERK) kinase (MEK) 1/2 inhibitor selumetinib versus temozolomide in chemotherapy-naive patients with unresectable stage III/IV melanoma.
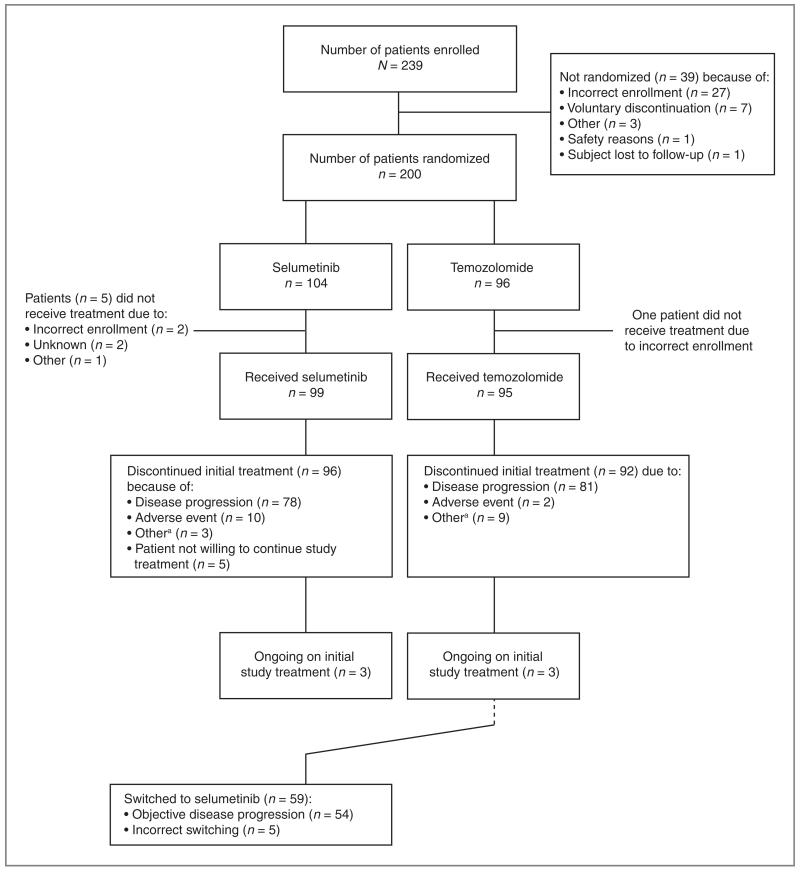
Experimental design: This phase II, open-label, multicenter, randomized, parallel-group study examined the effect of 100 mg oral selumetinib twice daily in 28-day cycles versus oral temozolomide (200 mg/m(2)/d for 5 days, then 23 days off-treatment). The primary endpoint was progression-free survival.
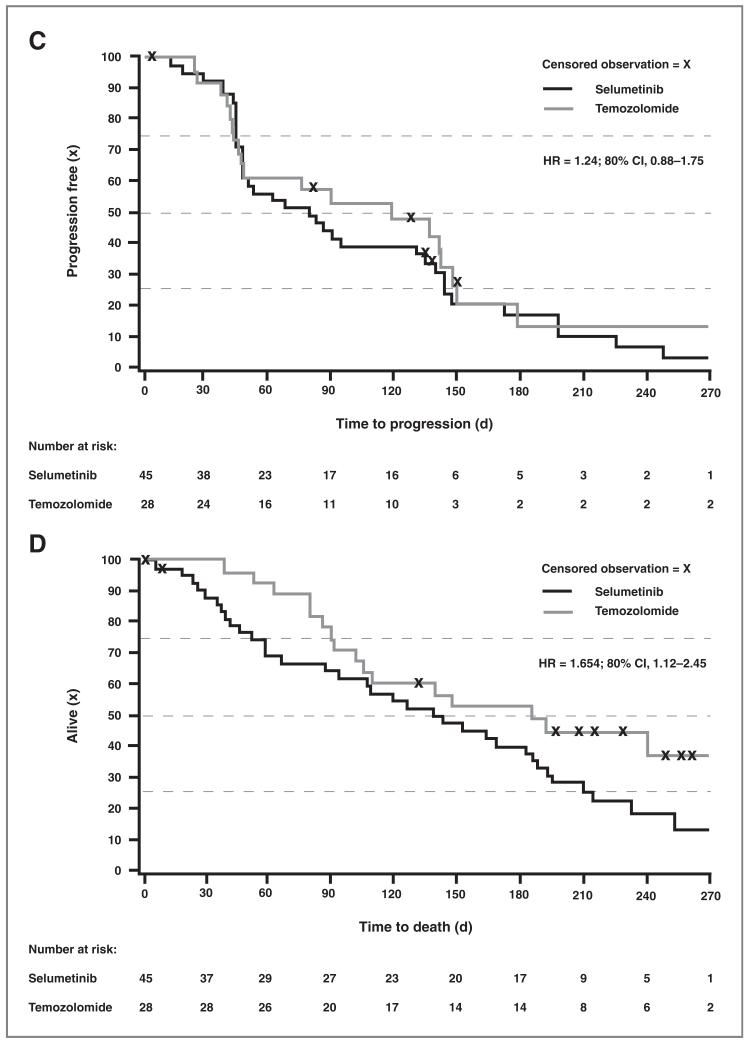
Results: Two hundred patients were randomized. Progression-free survival did not differ significantly between selumetinib and temozolomide (median time to event 78 and 80 days, respectively; hazard ratio, 1.07; 80% confidence interval, 0.86-1.32). Objective response was observed in six (5.8%) patients receiving selumetinib and nine (9.4%) patients in the temozolomide group. Among patients with BRAF mutations, objective responses were similar between selumetinib and temozolomide groups (11.1% and 10.7%, respectively). However, five of the six selumetinib partial responders were BRAF mutated. Frequently reported adverse events with selumetinib were dermatitis acneiform (papular pustular rash; 59.6%), diarrhea (56.6%), nausea (50.5%), and peripheral edema (40.4%), whereas nausea (64.2%), constipation (47.4%), and vomiting (44.2%) were reported with temozolomide.
Conclusions: No significant difference in progression-free survival was observed between patients with unresectable stage III/IV melanoma unselected for BRAF/NRAS mutations, who received therapy with selumetinib or temozolomide. Five of six patients with partial response to selumetinib had BRAF mutant tumors.
©2011 AACR.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
