

Comparative effectiveness evidence from the spine patient outcomes research trial: surgical versus nonoperative care for spinal stenosis, degenerative spondylolisthesis, and intervertebral disc herniation
- PMID: 22048651
- PMCID: PMC3472956
- DOI: 10.1097/BRS.0b013e318235457b
Comparative effectiveness evidence from the spine patient outcomes research trial: surgical versus nonoperative care for spinal stenosis, degenerative spondylolisthesis, and intervertebral disc herniation
Abstract
Study design: Cost-effectiveness analysis of a randomized plus observational cohort trial.
Objective: Analyze cost-effectiveness of Spine Patient Outcomes Research Trial data over 4 years comparing surgery with nonoperative care for three common diagnoses: spinal stenosis (SPS), degenerative spondylolisthesis (DS), and intervertebral disc herniation (IDH).
Summary of background data: Spine surgery rates continue to rise in the United States, but the safety and economic value of these procedures remain uncertain.
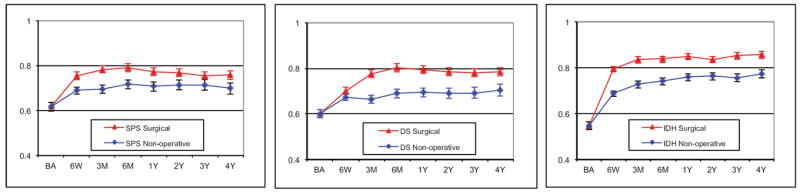
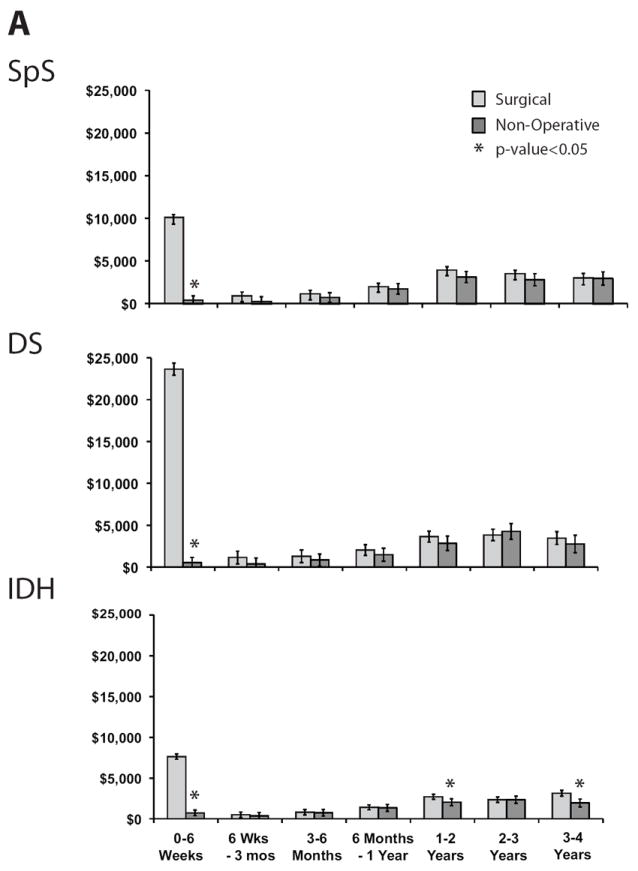
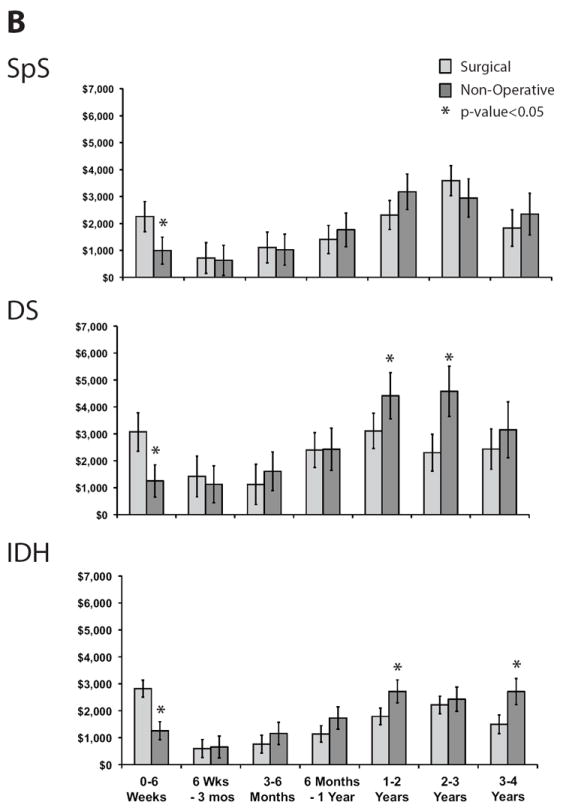
Methods: Patients with image-confirmed diagnoses were followed in randomized or observational cohorts with data on resource use, productivity, and EuroQol EQ-5D health state values measured at 6 weeks, 3, 6, 12, 24, 36, and 48 months. For each diagnosis, cost per quality-adjusted life year (QALY) gained in 2004 US dollars was estimated for surgery relative to nonoperative care using a societal perspective, with costs and QALYs discounted at 3% per year.
Results: Surgery was performed initially or during the 4-year follow-up among 414 of 634 (65.3%) SPS, 391 of 601 (65.1%) DS, and 789 of 1192 (66.2%) IDH patients. Surgery improved health, with persistent QALY differences observed through 4 years (SPS QALY gain 0.22; 95% confidence interval, CI: 0.15, 0.34; DS QALY gain 0.34, 95% CI: 0.30, 0.47; and IDH QALY gain 0.34, 95% CI: 0.31, 0.38). Costs per QALY gained decreased for SPS from $77,600 at 2 years to $59,400 (95% CI: $37,059, $125,162) at 4 years, for DS from $115,600 to $64,300 per QALY (95% CI: $32,864, $83,117), and for IDH from $34,355 to $20,600 per QALY (95% CI: $4,539, $33,088).
Conclusion: Comparative effectiveness evidence for clearly defined diagnostic groups from Spine Patient Outcomes Research Trial shows good value for surgery compared with nonoperative care over 4 years.
Figures
References
-
- Institute of Medicine. Initial National Priorities for Comparative Effectiveness Research. Washington, DC: National Academies Press; 2009.
-
- Dartmouth Atlas Working Group JW, PI. Dartmouth Atlas of Musculoskeletal Health Care. Chicago, IL: American Hospital Association Press; 2000.
-
- IOM (Institute of Medicine) Initial National Priorities for Comparative Effectiveness Research. Washington, D.C.: The National Academies Press; 2009.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
