

Ki-67: level of evidence and methodological considerations for its role in the clinical management of breast cancer: analytical and critical review
- PMID: 22048814
- PMCID: PMC3332349
- DOI: 10.1007/s10549-011-1837-z
Ki-67: level of evidence and methodological considerations for its role in the clinical management of breast cancer: analytical and critical review
Abstract
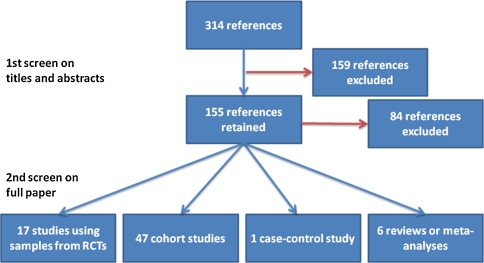
Clinicians can use biomarkers to guide therapeutic decisions in estrogen receptor positive (ER+) breast cancer. One such biomarker is cellular proliferation as evaluated by Ki-67. This biomarker has been extensively studied and is easily assayed by histopathologists but it is not currently accepted as a standard. This review focuses on its prognostic and predictive value, and on methodological considerations for its measurement and the cut-points used for treatment decision. Data describing study design, patients' characteristics, methods used and results were extracted from papers published between January 1990 and July 2010. In addition, the studies were assessed using the REMARK tool. Ki-67 is an independent prognostic factor for disease-free survival (HR 1.05-1.72) in multivariate analyses studies using samples from randomized clinical trials with secondary central analysis of the biomarker. The level of evidence (LOE) was judged to be I-B with the recently revised definition of Simon. However, standardization of the techniques and scoring methods are needed for the integration of this biomarker in everyday practice. Ki-67 was not found to be predictive for long-term follow-up after chemotherapy. Nevertheless, high KI-67 was found to be associated with immediate pathological complete response in the neoadjuvant setting, with an LOE of II-B. The REMARK score improved over time (with a range of 6-13/20 vs. 10-18/20, before and after 2005, respectively). KI-67 could be considered as a prognostic biomarker for therapeutic decision. It is assessed with a simple assay that could be standardized. However, international guidelines are needed for routine clinical use.
Figures
References
-
- Aleskandarany MA, Green AR, Rakha EA, Mohammed RA, Elsheikh SE, Powe DG, Paish EC, Macmillan RD, Chan S, Ahmed SI, Ellis IO. Growth fraction as a predictor of response to chemotherapy in node-negative breast cancer. Int J Cancer. 2010;126:1176–1761. - PubMed
-
- Andreetta C, Puppin C, Minisini A, Valent F, Pegolo E, Damante G, Di Loreto C, Pizzolitto S, Pandolfi M, Fasola G, Piga A, Puglisi F. Thymidine phosphorylase expression and benefit from capecitabine in patients with advanced breast cancer. Ann Oncol. 2009;20:265–271. doi: 10.1093/annonc/mdn592. - DOI - PubMed
-
- Assersohn L, Salter J, Powles TJ, A’Hern R, Makris A, Gregory RK, Chang J, Dowsett M. Studies of the potential utility of Ki67 as a predictive molecular marker of clinical response in primary breast cancer. Breast Cancer Res Treat. 2003;82:113–123. doi: 10.1023/B:BREA.0000003968.45511.3f. - DOI - PubMed
-
- Bartlett JMS, Munro A, Cameron Da, Thomas J, Prescott R, Twelves CJ. Type 1 receptor tyrosine kinase profiles identify patients with enhanced benefit from anthracyclines in the BR9601 Adjuvant Breast Cancer Chemotherapy Trial. J Clin Oncol. 2008;26:5027–5035. doi: 10.1200/JCO.2007.14.6597. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
