

A cost-effectiveness analysis of a preventive exercise program for patients with advanced head and neck cancer treated with concomitant chemo-radiotherapy
- PMID: 22051143
- PMCID: PMC3237585
- DOI: 10.1186/1471-2407-11-475
A cost-effectiveness analysis of a preventive exercise program for patients with advanced head and neck cancer treated with concomitant chemo-radiotherapy
Abstract
Background: Concomitant chemo-radiotherapy (CCRT) has become an indispensable organ, but not always function preserving treatment modality for advanced head and neck cancer. To prevent/limit the functional side effects of CCRT, special exercise programs are increasingly explored. This study presents cost-effectiveness analyses of a preventive (swallowing) exercise program (PREP) compared to usual care (UC) from a health care perspective.
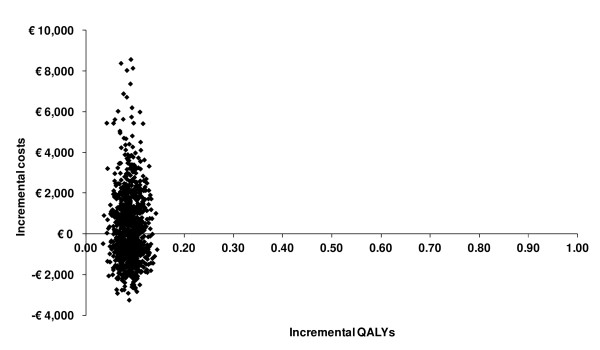
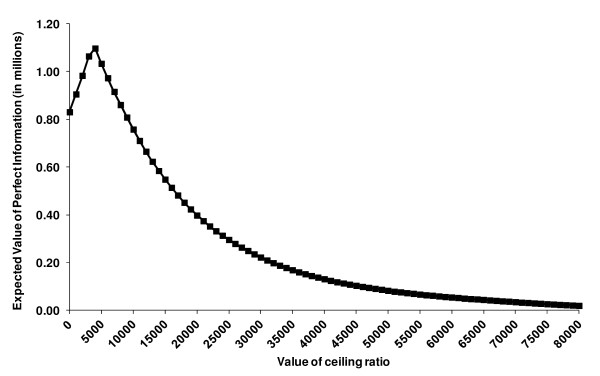
Methods: A Markov decision model of PREP versus UC was developed for CCRT in advanced head and neck cancer. Main outcome variables were tube dependency at one-year and number of post-CCRT hospital admission days. Primary outcome was costs per quality adjusted life years (cost/QALY), with an incremental cost-effectiveness ratio (ICER) as outcome parameter. The Expected Value of Perfect Information (EVPI) was calculated to obtain the value of further research.
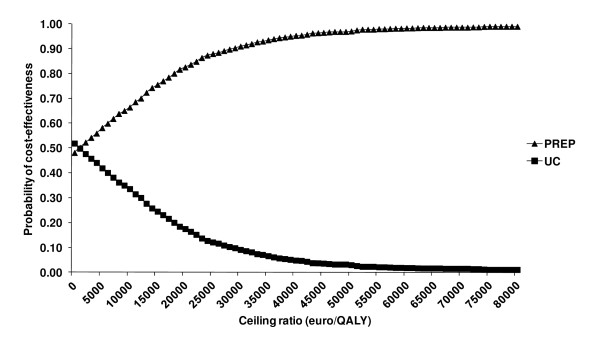
Results: PREP resulted in less tube dependency (3% and 25%, respectively), and in fewer hospital admission days than UC (3.2 and 4.5 days respectively). Total costs for UC amounted to €41,986 and for PREP to €42,271. Quality adjusted life years for UC amounted to 0.68 and for PREP to 0.77. Based on costs per QALY, PREP has a higher probability of being cost-effective as long as the willingness to pay threshold for 1 additional QALY is at least €3,200/QALY. At the prevailing threshold of €20,000/QALY the probability for PREP being cost-effective compared to UC was 83%. The EVPI demonstrated potential value in undertaking additional research to reduce the existing decision uncertainty.
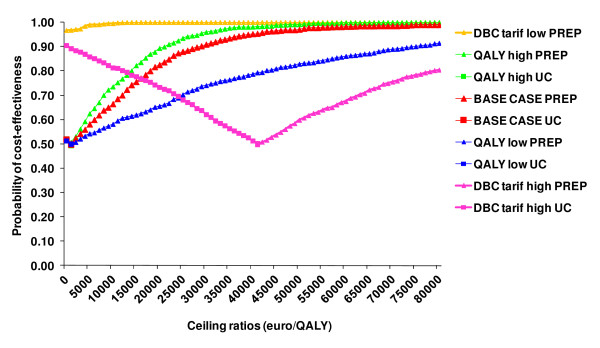
Conclusions: Based on current evidence, PREP for CCRT in advanced head and neck cancer has the higher probability of being cost-effective when compared to UC. Moreover, the majority of sensitivity analyses produced ICERs that are well below the prevailing willingness to pay threshold for an additional QALY (range from dominance till €45,906/QALY).
Figures
References
-
- Van der Molen L, van Rossum MA, Burkhead LM, Smeele LE, Hilgers FJ. Functional outcomes and rehabilitation strategies in patients treated with chemoradiotherapy for advanced head and neck cancer: a systematic review. Eur Arch Otorhinolaryngol. 2009;266(6):901–2. doi: 10.1007/s00405-008-0845-z. - DOI - PubMed
-
- Kreeft A, Tan IB, van den Brekel MW, Hilgers FJ, Balm AJ. The surgical dilemma of 'functional inoperability' in oral and oropharyngeal cancer: current consensus on operability with regard to functional results. Clin Otolaryngol. 2009;34(2):140–6. doi: 10.1111/j.1749-4486.2009.01884.x. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
