

Impaired natriuretic and renal endocrine response to acute volume expansion in pre-clinical systolic and diastolic dysfunction
- PMID: 22051332
- PMCID: PMC3835631
- DOI: 10.1016/j.jacc.2011.07.042
Impaired natriuretic and renal endocrine response to acute volume expansion in pre-clinical systolic and diastolic dysfunction
Abstract
Objectives: We hypothesized an impaired renal endocrine and natriuretic response to volume expansion (VE) in humans with pre-clinical systolic dysfunction (PSD) and pre-clinical diastolic dysfunction (PDD). We further hypothesized that exogenous B-type natriuretic peptide (BNP) could rescue an impaired natriuretic response in PSD and PDD.
Background: Recent reports suggest that in early systolic heart failure (HF), there is an impaired natriuretic response to acute VE.
Methods: PSD was defined as left ventricular ejection fraction <40% without HF symptoms. PDD was defined as ejection fraction >50%, moderate to severe diastolic dysfunction by Doppler criteria, and no HF symptoms. A double-blinded, placebo-controlled, crossover study was employed to determine the renal response to VE (0.25 ml/kg/min of normal saline for 60 min) in the presence and absence of exogenous BNP. Twenty healthy control subjects, 20 PSD subjects, and 18 PDD subjects participated.
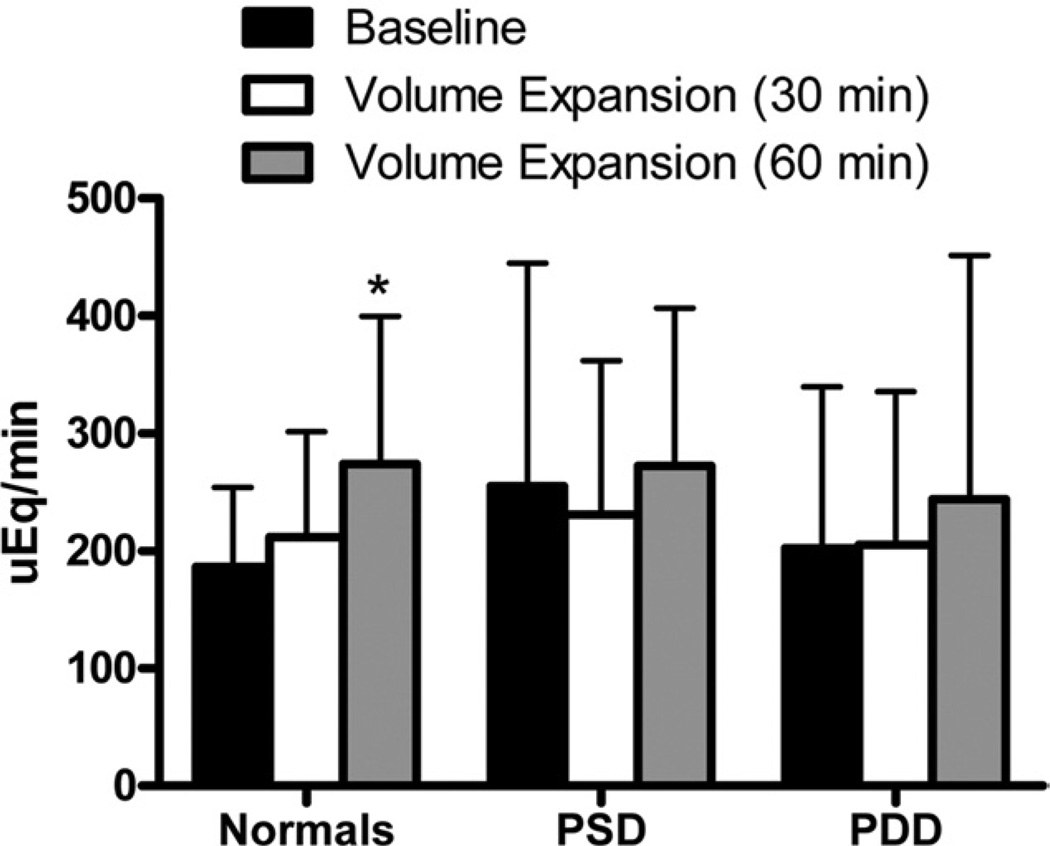
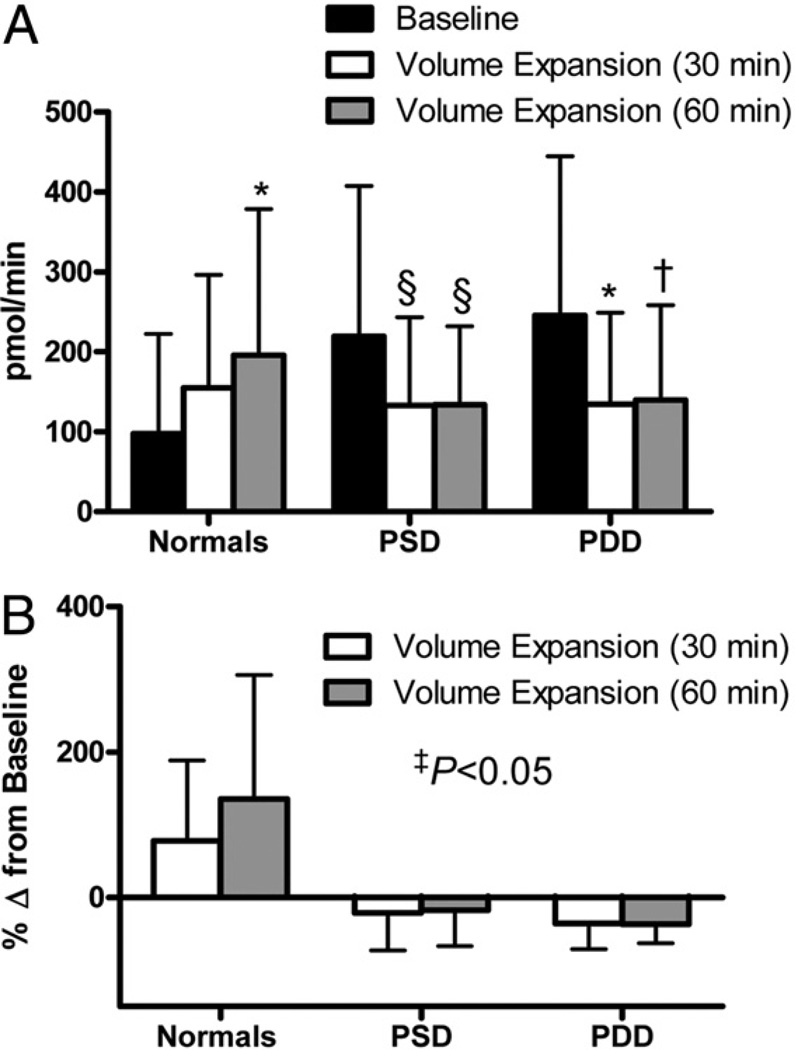
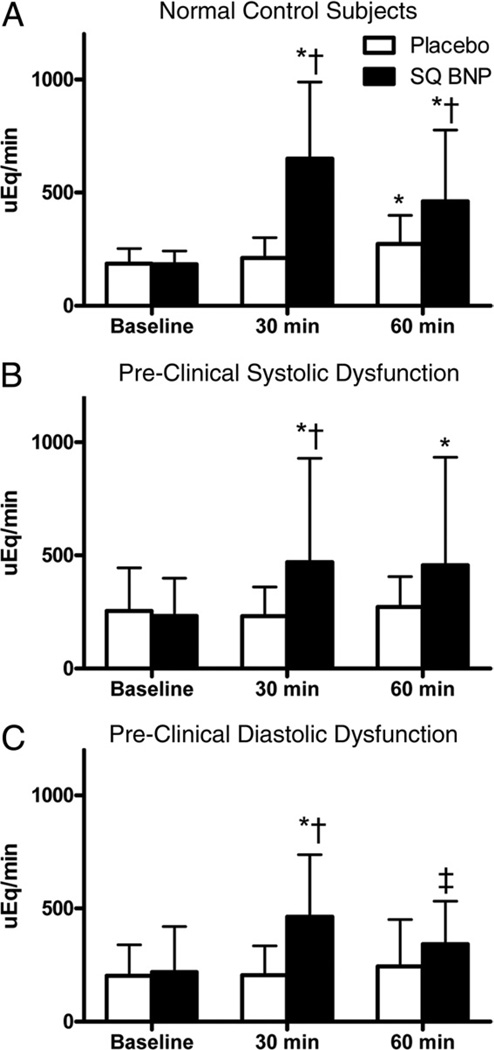
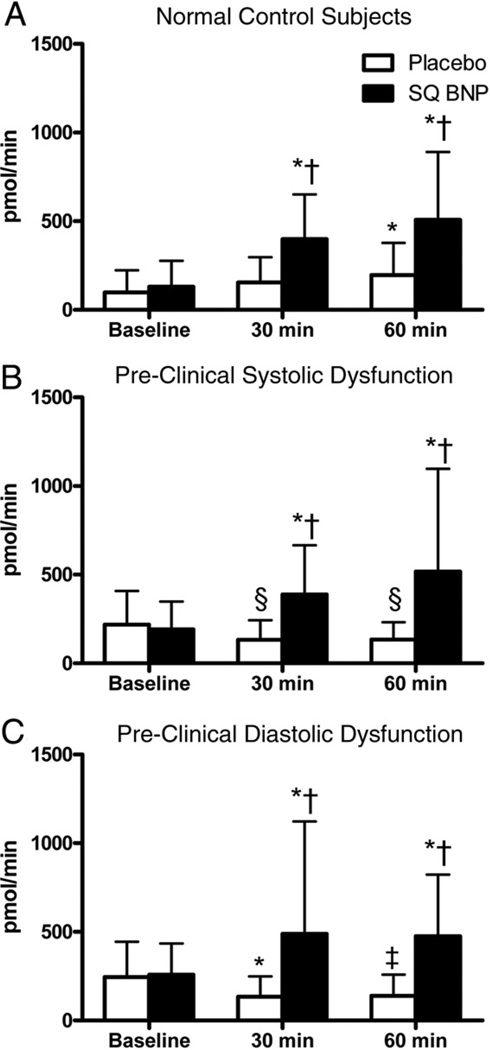
Results: In healthy control subjects, urinary cyclic guanosine monophosphate (cGMP) and natriuresis increased after VE. In contrast, among PSD and PDD subjects, there was a paradoxical decrease in urinary cGMP and attenuated natriuresis. Pre-treatment with subcutaneous BNP resulted in similar increases in both urinary cGMP and natriuresis among healthy normal, PSD, and PDD subjects.
Conclusions: In PSD and PDD, there is impaired renal cGMP activation, which contributes to impaired natriuresis in response to VE. Impaired activation of urinary cGMP and reduced natriuresis may contribute to volume overload and the progression of HF among PSD and PDD subjects. Importantly, the impaired renal excretory response to VE is rescued by exogenous BNP in PSD and PDD.
Copyright © 2011 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
The early intertwining of the heart and the kidney through an impaired natriuretic response to acute volume expansion.J Am Coll Cardiol. 2011 Nov 8;58(20):2104-5. doi: 10.1016/j.jacc.2011.05.064. J Am Coll Cardiol. 2011. PMID: 22051333 No abstract available.
References
-
- Jessup M, Abraham WT, Casey DE, et al. 2009 focused update: ACCF/AHA guidelines for the diagnosis and management of heart failure in adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2009;53:1343–1382. - PubMed
-
- Wang TJ, Evans JC, Benjamin EJ, Levy D, LeRoy EC, Vasan RS. Natural history of asymptomatic left ventricular systolic dysfunction in the community. Circulation. 2003;108:977–982. - PubMed
-
- Volpe M, Tritto C, DeLuca N, et al. Abnormalities of sodium handling and of cardiovascular adaptations during high salt diet in patients with mild heart failure. Circulation. 1993;88:1620–1627. - PubMed
-
- Senni M, Tribouilloy CM, Rodeheffer RJ, et al. Congestive heart failure in the community: a study of all incident cases in Olmsted County, Minnesota, in 1991. Circulation. 1998;98:2282–2289. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
