

Impact of practice patterns in shunt use during carotid endarterectomy with contralateral carotid occlusion
- PMID: 22051863
- PMCID: PMC3243768
- DOI: 10.1016/j.jvs.2011.07.046
Impact of practice patterns in shunt use during carotid endarterectomy with contralateral carotid occlusion
Abstract
Purpose: This study investigated the association between surgeon practice pattern in shunt placement and 30-day stroke/death in patients undergoing carotid endarterectomy (CEA) with contralateral carotid occlusion (CCO).
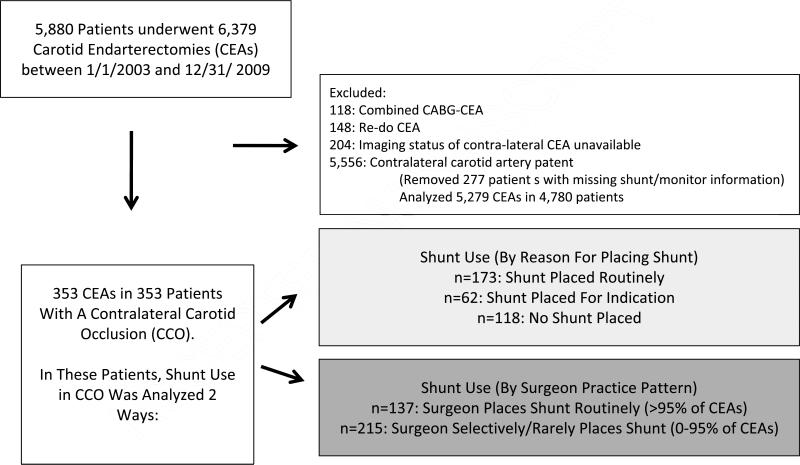
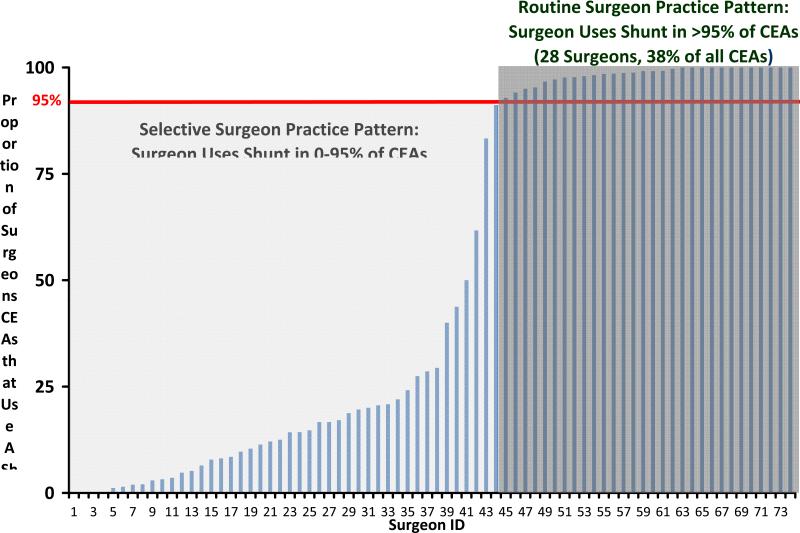
Methods: Among 6379 CEAs performed in the Vascular Study Group of New England (VSGNE) between 2002 and 2009, we identified 353 patients who underwent CEA with CCO and compared the 30-day stroke/death rate with 5279 patients who underwent primary, isolated CEA with a patent contralateral carotid artery. Within patients with CCO, we examined the 30-day stroke/death rate across the reason for shunt placement and two distinct surgeon practice patterns in shunt placement: surgeons who selectively used a shunt (≤95% of CEAs) or routinely used a shunt (>95% of CEAs). We used observed/expected (O/E) ratios to provide risk-adjusted comparisons across groups.
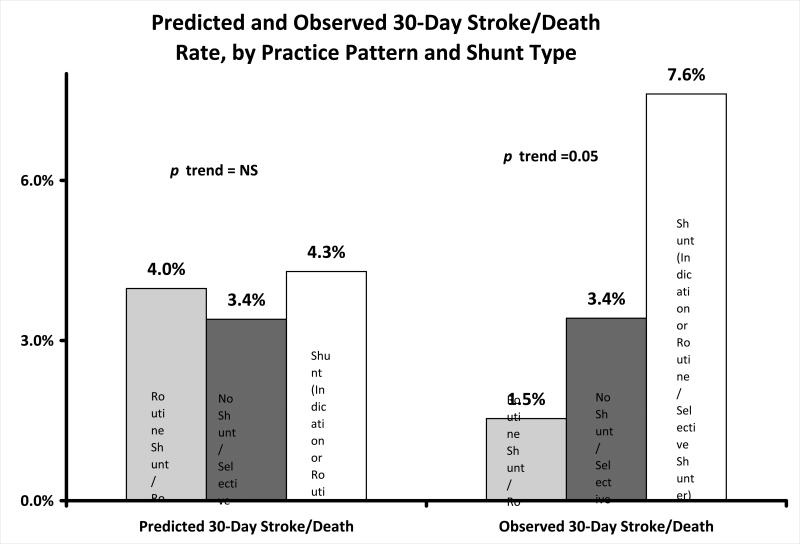
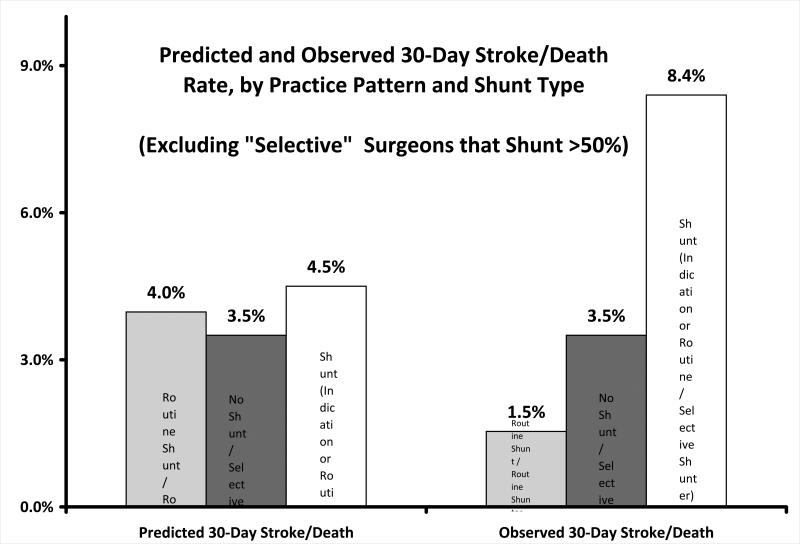
Results: Of 353 patients with CCO, 118 (33%) underwent CEA without a shunt, 173 (49%) underwent CEA using a shunt placed routinely, and 62 (18%) had a shunt placed for a neurologic indication. Rates of 30-day stroke/death across categories of reason for shunt use were no shunt, 3.4%; routine shunt, 4.0%; and shunt for indication, 4.8% (P = .891). The risk of 30-day stroke/death was higher for surgeons who selectively placed shunts (5.6%) in all their CEAs and lower for surgeons who routinely placed shunts (1.5%, P = .05). The risk of 30-day stroke/death was >1 in patients undergoing selective shunting (O/E ratio, 1.4; 95% confidence interval [CI], 1.1-1.7) and <1 for surgeons who placed shunts routinely (O/E ratio, 0.4; 95% CI, 0.2-0.9). Stroke/death rates were lowest when individual surgeons' intraoperative decisions reflected their usual pattern of practice: 1.5% stroke/death rate when "routine" surgeons placed a shunt, 3.4% when "selective" surgeons did not place a shunt, and 7.6% stroke/death rate for "selective" surgeons who placed a shunt (P = .05 for trend).
Conclusions: The risk of 30-day stroke/death is higher in CEA in patients with CCO than with a patent contralateral carotid artery. Surgeons who place shunts selectively during CEA have higher rates of stroke/death in patients with CCO. This suggests that shunt use for CCO during CEA is associated with fewer complications, but only if the surgeon uses a shunt as part of his or her routine practice in CEA. Surgeons should preoperatively consider their own practice pattern in shunt use when faced with a patient who may require shunt placement.
Copyright © 2012 Society for Vascular Surgery. Published by Mosby, Inc. All rights reserved.
Figures
Comment in
-
Regarding "Impact of practice patterns in shunt use during carotid endarterectomy with contralateral carotid occlusion".J Vasc Surg. 2012 Jun;55(6):1838; author reply 1838. doi: 10.1016/j.jvs.2012.02.045. J Vasc Surg. 2012. PMID: 22608050 No abstract available.
References
-
- Adelman MA, Jacobowitz GR, Riles TS, et al. Carotid endarterectomy in the presence of a contralateral occlusion: a review of 315 cases over a 27-year experience. Cardiovasc Surg. 1995;3:307–12. - PubMed
-
- Jacobowitz GR, Adelman MA, Riles TS, Lamparello PJ, Imparato AM. Long-term follow-up of patients undergoing carotid endarterectomy in the presence of a contralateral occlusion. American Journal of Surgery. 1995;170:165–7. - PubMed
-
- Julia P, Chemla E, Mercier F, Renaudin JM, Fabiani JN. Influence of the status of the contralateral carotid artery on the outcome of carotid surgery. Annals of Vascular Surgery. 1998;12:566–71. - PubMed
-
- Samson RH, Showalter DP, Yunis JP. Routine carotid endarterectomy without a shunt, even in the presence of a contralateral occlusion. Cardiovasc Surg. 1998;6:475–84. - PubMed
-
- Ballotta E, Saladini M, Gruppo M, Mazzalai F, Da Giau G, Baracchini C. Predictors of electroencephalographic changes needing shunting during carotid endarterectomy. Annals of Vascular Surgery. 2010;24:1045–52. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
