

Guided medication dosing for elderly emergency patients using real-time, computerized decision support
- PMID: 22052899
- PMCID: PMC3240752
- DOI: 10.1136/amiajnl-2011-000124
Guided medication dosing for elderly emergency patients using real-time, computerized decision support
Abstract
Objective: To evaluate the impact of a real-time computerized decision support tool in the emergency department that guides medication dosing for the elderly on physician ordering behavior and on adverse drug events (ADEs).
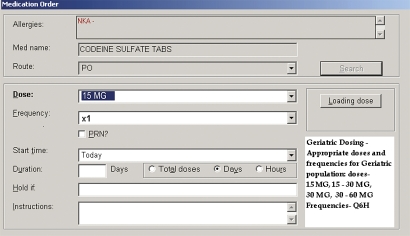
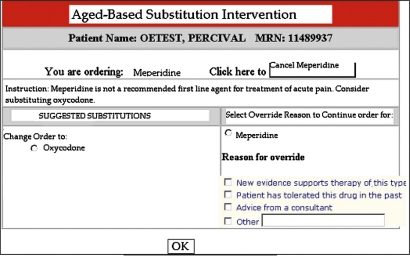
Design: A prospective controlled trial was conducted over 26 weeks. The status of the decision support tool alternated OFF (7/17/06-8/29/06), ON (8/29/06-10/10/06), OFF (10/10/06-11/28/06), and ON (11/28/06-1/16/07) in consecutive blocks during the study period. In patients ≥65 who were ordered certain benzodiazepines, opiates, non-steroidals, or sedative-hypnotics, the computer application either adjusted the dosing or suggested a different medication. Physicians could accept or reject recommendations.
Measurements: The primary outcome compared medication ordering consistent with recommendations during ON versus OFF periods. Secondary outcomes included the admission rate, emergency department length of stay for discharged patients, 10-fold dosing orders, use of a second drug to reverse the original medication, and rate of ADEs using previously validated explicit chart review.
Results: 2398 orders were placed for 1407 patients over 1548 visits. The majority (49/53; 92.5%) of recommendations for alternate medications were declined. More orders were consistent with dosing recommendations during ON (403/1283; 31.4%) than OFF (256/1115; 23%) periods (p≤0.0001). 673 (43%) visits were reviewed for ADEs. The rate of ADEs was lower during ON (8/237; 3.4%) compared with OFF (31/436; 7.1%) periods (p=0.02). The remaining secondary outcomes showed no difference.
Limitations: Single institution study, retrospective chart review for ADEs.
Conclusion: Though overall agreement with recommendations was low, real-time computerized decision support resulted in greater acceptance of medication recommendations. Fewer ADEs were observed when computerized decision support was active.
Conflict of interest statement
Figures
References
-
- Administration on Aging Profile of Older Americans: 2010. http://www.aoa.gov/aoaroot/aging_statistics/Profile/2010/2.aspx (accessed Jul 2011).
-
- Shelton PS, Fritsch MA, Scott MA. Assessing medication appropriateness in the elderly: a review of available measures. Drugs Aging 2000;16:437–50 - PubMed
-
- McCaig LF, Stussman BJ. National Hospital Ambulatory Medical Care Survey: 1996 emergency department summary. Adv Data 1997;293:1–20 - PubMed
-
- Nawar EW, Niska RW, Xu J. National Hospital Ambulatory Medical Care Survey: 2005 emergency department summary. Adv Data 2007;386:1–32 - PubMed
-
- Hohl CM, Dankoff J, Colacone A, et al. Polypharmacy, adverse drug-related events, and potential adverse drug interactions in elderly patients presenting to an emergency department. Ann Emerg Med 2001;38:666–71 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
