

A proposal: Atopic Dermatitis Organizer (ADO) guideline for children
- PMID: 22053298
- PMCID: PMC3206255
- DOI: 10.5415/apallergy.2011.1.2.53
A proposal: Atopic Dermatitis Organizer (ADO) guideline for children
Abstract
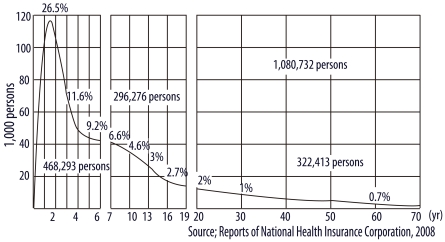
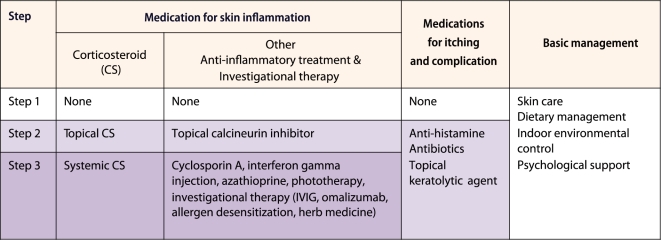
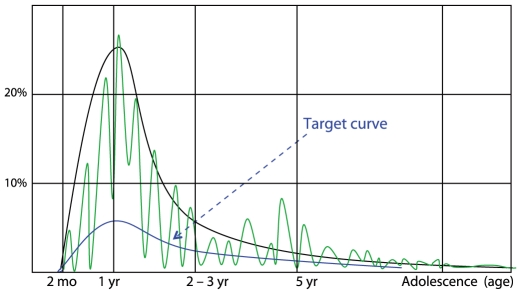
Atopic dermatitis (AD) is the most common chronic inflammatory skin disorder in children, with a worldwide cumulative prevalence in children of 8-20%. The number of AD patients is beyond the level that can be dealt with at clinics and it is time to make an effort to reduce the number of AD patients in the community. Thus, caregivers and all persons involved with AD management, including health care providers, educators, technologists and medical policy makers, should understand the development and the management of AD. Although a number of guidelines such as Practical Allergy (PRACTALL) report have been developed and used, community understanding of these is low. This is probably because there are still remarkable differences in management practices between specialists and between countries and most of the reported guidelines have been prepared for physicians. From the viewpoint of providing a basis for a multidisciplinary team approach, easily comprehensible guidelines for organizing treatment of AD, i.e. an Atopic Dermatitis Organizer (ADO), are required. guidelines should be simple and well organized. We suggest an easy approach with a new classification of AD symptoms into early and/or progressive lesions in acute and/or chronic symptoms. The contents of this ADO guideline basically consist of 3 steps approaches: conservative management, topical anti-inflammatory therapy, and systemic anti-inflammatory therapy.
Keywords: Atopic dermatitis; Guideline; classification, Management.
Figures
References
-
- Johansson SG, Hourihane JO, Bousquet J, Bruijnzeel-Koomen C, Dreborg S, Haahtela T, Kowalski ML, Mygind N, Ring J, van Cauwenberge P, van Hage-Hamsten M, Wüthrich B. A revised nomenclature for allergy. An EAACI position statement from the EAACI nomenclature task force. Allergy. 2001;56:813–824. - PubMed
-
- Purvis DJ, Thompson JM, Clark PM, Robinson E, Black PN, Wild CJ, Mitchell EA. Risk factors for atopic dermatitis in New Zealand children at 3.5 years of age. Br J Dermatol. 2005;152:742–749. - PubMed
-
- Asher MI, Montefort S, Björkstén B, Lai CK, Strachan DP, Weiland SK, Williams H ISAAC Phase Three Study Group. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross-sectional surveys. Lancet. 2006;368:733–743. - PubMed
-
- Williams H, Stewart A, von Mutius E, Cookson W, Anderson HR International Study of Asthma and Allergies in Childhood (ISAAC) Phase One and Three Study Groups. Is eczema really on the increase worldwide? J Allergy Clin Immunol. 2008;121:947–954. - PubMed
-
- Lee JH, Kim EH, Cho JB, Kim HY, Suh JM, Ahn KM, Cheong HK, Lee SI. Comparison of prevalence and risk factors of atopic dermatitis by physical examination and questionnaire survey in elementay school children. Pediatr Allergy Respir Dis. 2011 (Unpublished data)
LinkOut - more resources
Full Text Sources